


vaccine induced cancer and SV40 DNA
Pfizer admits SV40 DNA plasmids are "common practice" in vaccine development after concealing it from regulators


So they admit it and are lying about the DNA contamination which is proven which I will demonstrate. I said they were all contaminated and they are. FDA/EMA/Health Canada were aware of these issues for the convid quacksine and failed to warn the public as brilliantly exposed by Rebel News.
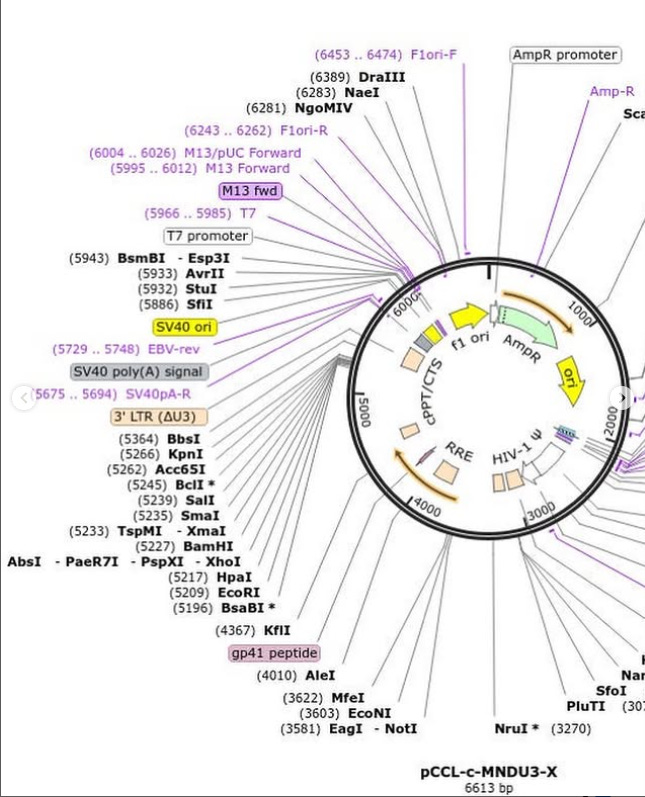
I have previously shown Pfizer deliberately deleted the annotation of the SV40 promoter.
Pfizer is correct when they say SV40 has been used in vaccine development for decades. Here are some examples:



It is true and has been published in the literature for decades. So what gave them this great idea to use cancer causing monkey viruses in vaccines?
Few back then grasped that these vaccines might also be a huge, inadvertent, uncontrolled experiment in interspecies viral transmission. But from 1955 to 1963, according to a 1976 US National Institutes of Health (NIH)-funded study, 98 million Americans alone probably were exposed to polio vaccines contaminated with SV40—a monkey virus that can cause cancers in animals. Now, a July 7 report in New Scientist has raised fears that hundreds of millions of eastern Europeans, Asians, and Africans also may have been exposed to SV40 in Soviet-made polio vaccines. Michele Carbone of Loyola University Medical Center, Chicago, USA, announced at the 2004 Vaccine Cell Substrates meeting (Rockville, MD) that the Soviet vaccine could have been contaminated until the 1980s. This is worrying since, despite 44 years of medical debate, epidemiological studies have yet to establish conclusively whether SV40 has or hasn't caused cancers in people.
When Salk developed his vaccine, instead of using human tissues, as did the scientists who won a Nobel Prize for first growing poliovirus in tissue culture, he used minced-up rhesus macaque monkey kidneys, which were remarkably efficient poliovirus factories. Those who sought to supplant Salk's formaldehyde-inactivated vaccine with live, attenuated oral vaccine also used monkey kidney cultures. Despite a manufacturing problem that, at best, left six children who received the vaccine paralysed in the arm, and despite concerns about wild simian viruses, Salk's shots were declared safe and effective after 1954 field trials. The next year, after grudging approval by sceptical government regulators, free Salk shots were made available throughout the USA.
By 1960, scientists and vaccine manufacturers knew that monkey kidneys were sewers of simian viruses. Such contamination often spoiled cultures, including those of an NIH researcher named Bernice Eddy, who worked on vaccine safety. In 1959, fresh from co-reporting that the mouse polyoma virus could cause cancer in other animals, Eddy tested the rhesus monkey kidney substrate used to make polio vaccine. She injected 154 newborn hamsters with extracts of the cell cultures: 109 developed tumours. Next, she ground up three of the tumours and injected the residue into other hamsters. The animals receiving injections from two of the three tumours developed cancers. But when Eddy put the substance back into the monkey cell culture, nothing happened, and she couldn't isolate the suspected virus.
In The Virus and the Vaccine: The True Story of a Cancer-Causing Monkey Virus, Contaminated Polio Vaccine, and the Millions of Americans Exposed, Debbie Bookchin and Jim Schumacher report that in 1960, when Eddy presented her results to her boss, a polio vaccine champion named Joe Smadel, he was livid and disbelieving: “Its implications—that something in the polio vaccine could cause cancer—was an affront to his career.” Her discovery also threatened one of the USA's most important public-health programmes. “By 1960, tens of millions of Americans had been vaccinated against polio, and it was federal health policy that everyone should be vaccinated and continue to receive Salk booster shots.”
Eddy tried to get word out to colleagues but was muzzled and stripped of her vaccine regulatory duties and her laboratory. However, two Merck researchers, Ben Sweet and Maurice Hilleman, soon identified the rhesus virus later named SV40—the carcinogenic agent that had eluded Eddy. In 1963, US authorities decided to switch to African green monkeys, which are not natural hosts of SV40, to produce polio vaccine. In the mid-1970s, after limited epidemiological studies, authorities concluded that although SV40 caused cancer in hamsters, it didn't seem to do so in people.
Fast forward to the 1990s: Michele Carbone, then at NIH, was working on how SV40 induces cancers in animals. One of these was mesothelioma, a rare cancer of the pleura thought in people to be caused mainly by asbestos. The orthodoxy held that SV40 didn't cause human cancers. Emboldened by a 1992 NEJM paper that found DNA “footprints” of SV40 in childhood brain tumours, Carbone tested human mesothelioma tumour biopsies at the National Cancer Institute: 60% contained SV40 DNA. In most, the monkey virus was active and producing proteins.
He published his results in Oncogene in May, 1994, but the NIH declined to publicise them. Doubters at NIH developed epidemiological evidence that showed no correlation between people who received potentially contaminated polio vaccines and increased cancer rates. Others suggested that the SV40 DNA was a laboratory contaminant. On the first point, the US Institute of Medicine reviewed all published epidemiological studies of SV40 and found them inconclusive. Meanwhile, Carbone had moved to Loyola University. There he discovered how SV40 disables tumour suppressor genes in human mesothelioma, and published his results in Nature Medicine in July, 1997. Studies in Italy, Germany, and the USA also showed associations between SV40 and human cancers.
Between 1997 and early 2003, say Bookchin and Schumacher, more than 25 published studies found SV40 in human mesotheliomas; 16 others found the virus in brain and bone cancers, lymphomas, and other cancers and in kidneys and peripheral blood. As of 2003, SV40 had been found in human tumours in 18 developed countries. Bookchin and Schumacher claim that the rates of SV40-positive tumours seem highest in countries that used the greatest amount of contaminated Salk polio vaccine, including the UK, USA, and Italy.
As the SV40 story illustrates, until scientists know that a virus exists in cell cultures, they can't create a test to detect it and thus can't eliminate it from vaccines grown on those cultures. Might other potentially dangerous simian viruses lurk in primary monkey kidney cultures used for polio vaccines? Such concerns were relieved in January, 2000, when attenuated oral polio vaccine made since the 1950s by Lederle Laboratories on primary monkey kidney cultures was removed from the US market. Since wild-type polio cases had been eradicated in the USA in the mid-1970s, the eight to ten cases of paralysis caused yearly by return to neurovirulence of the live vaccine virus were finally deemed no longer acceptable. The vaccine was replaced with Aventis Pasteur's killed polio vaccine grown on a well characterised VERO monkey cell line. Thus the odds of further contamination by unrecognised viruses are thought to have been greatly reduced.
Bookchin and Schumacher complain that since the era of Bernice Eddy the NIH hierarchy has been consistently dismissive of evidence that SV40 from vaccines may have caused human cancers. Officials who had previously said SV40 was harmless were authorised to assess independent research that challenged that conclusion: “Not surprisingly, they reaffirmed their own previous wisdom.” Accepting that SV40 is a human carcinogen, they continue, raises questions about what the government response should be: “A coordinated and extensive search for SV40 in other kinds of tumors, coupled with far greater efforts to study how the virus causes tumors? A crash SV40 screening program among populations most likely to have been infected? … An anti-SV40 vaccination campaign?” The problem, they continue, is that to undertake any of these options the government would have to admit that it should have acted sooner to protect public health.
In The Structure of Scientific Revolutions (University of Chicago Press, 1962) Thomas Kuhn suggests that paradigm shifts don't happen because opponents are converted by evidence, but rather because one generation of investigators and scientific leaders dies and is replaced by another. For credible epidemiological studies confirming whether SV40 from polio vaccines has caused human cancers, we may have to wait until a new generation is put in charge of the USA's health research bureaucracy.
So where did this all begin? It begins with “what about polio?”. Dr. Jack Kruse does a great job telling the story.
Shannon Joy made an excellent documentary about this history as well:
I will let the pro-vaxx Institute of Medicine resume the story with their confession:

The IoM is a biased source of information. Other papers were more honest and said it outright.


three independent scientific panels have all agreed that there is compelling evidence that SV40 is present in some human cancers and that SV40 could contribute to the pathogenesis of some of them. It should be noted that the presence of SV40 in mesothelioma and other human tumor types has been challenged by a research team that has consistently reported negative findings (Strickler et al., 2001). However, a member of this research team has recently acknowledged - in sworn testimony -sensitivity problems and possible irregularities that raise concerns about these negative reports (MacLachlan, 2002). These revelations, together with the conclusions of the three independent panels mentioned above, appear to bring to an end the apparent controversy about the presence of SV40 in human mesotheliomas and brain tumors. source
SV40 has been detected in human tumors in over 40 different labs?!
This paper is current and it is to show SV40 is still causing mesothelioma
We all know it causes myopericarditis and you just read SV40 can cause mesothelioma. Well now that pericarditis could really be a mesothelioma mass. The patient died 3 weeks later. So much for mild and temporary.
I wonder how many will find the Pfizer SV40 sequence in the tumour biopsies like Kevin Mckernan did?
Persuasive evidence indicates SV40 is causing cancer today. I will focus on hematological or blood cancers lymphoma and leukemia.

So the polio vaccine that they worship the most was contaminated with SV40 from monkey kidney cells that “has biological properties consistent with a cancer-causing virus”. Seems like a pretty big mistake. One would think they would do everything in their power to never again use monkey kidney cells and ensure their products are free of residual DNA and SV40 right?…

They did the exact opposite. SV40 was used in “gene therapy” research and a whole cell line from the kidneys of African Green Monkeys infected with SV40 called VERO cells were widely used in vaccine development.

See Dr. Tenpenny’s substack for the vile abominations they use to make vaccines with.

Today, VERO cells from African Green Monkeys, are used to manufacture the following vaccines:
Polio (Inactivated), Hepatitis A, Mumps, Yellow Fever, Zika, Rabies, Dengue, Japanese Encephalitis, Ebola, Avian influenza (bird flu), and Chikungunya (investigational).
Seriously who thinks of this stuff. It is pretty clearly witchcraft.
Why not just use human tumors to make vaccines?! FDA says great idea.
No wonder they wont test for oncogenesis in section 13.
From the same document:
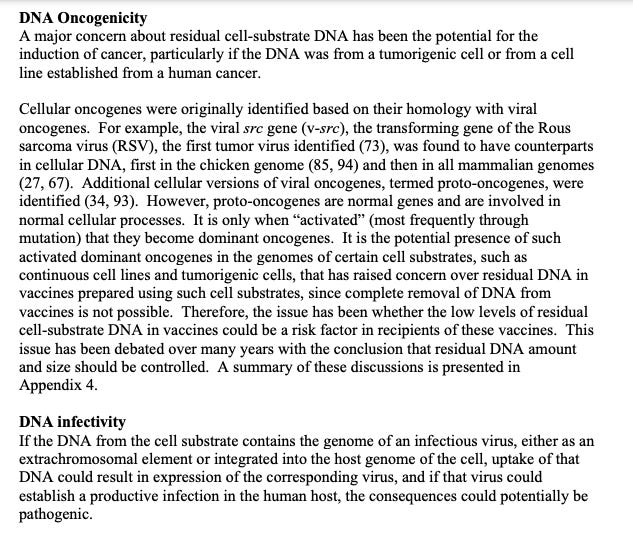
DNA has the potential for the induction of cancer…Good to know.
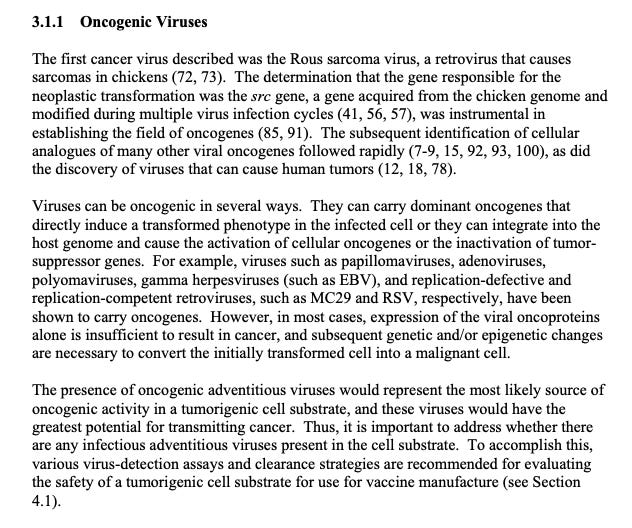
Notice EBV is listed as an oncogenic virus. We will be coming back to that in the lymphoma section.

Somatic Mutations. Where have I heard that before? Oh yeah. This one.
AID (activation-induced cytidine deaminase), a member of the APOBEC family, is the initiator of the antibody diversification process known as somatic hypermutation and its aberrant expression and targeting is a frequent source of lymphomagenesis. In this study, we investigated whether AID could cause mutations in SV40 LT. We demonstrate that the SV40 enhancer has strong somatic hypermutation targeting activity in several cell types and that AID-induced mutations accumulate in SV40 LT in B cells and kidney cells and cause truncated LT expression in B cells. Our results argue that the ability of the SV40 enhancer to target somatic hypermutation to LT is a potential source of LT truncation events that could contribute to tumorigenesis in various cell types, thereby linking SV40 infection with malignant development through a novel mutagenic pathway. source

The “issue” of DNA in vaccines is cancer…and its infectious.

This source is to show the whole SV40 is not required for nuclear import. Just the 72 base pair SV40 cancer enhancer.
source Again only the DNA Nuclear Targeting Sequence is required.
From the FDA guidance for industry source
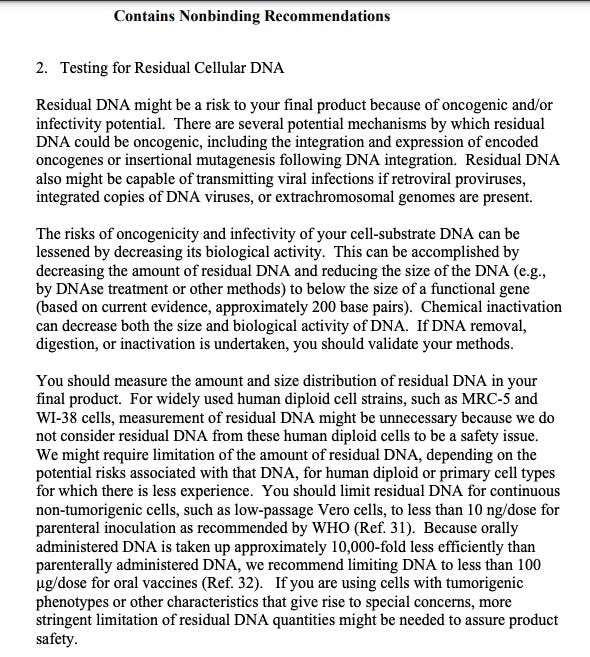
It is clear the FDA, Moderna and Pfizer knew residual DNA and SV40 promoters are a cancer risk.
The DNA template used in the mRNA manufacturing process must be removed to ensure the efficacy of therapeutics and safety, because residual DNA in drug products may induce activation of the innate response and has the potential to be oncogenic in patient populations. Regulatory guidelines may also require the quantification, control, and removal of the DNA template in RNA products. Currently available or reported methods do not address this deficiency. source
The direct injection of genetically engineered DNA (e.g., naked plasmid DNA) into a living host results in a small number of its cells directly producing an antigen, resulting in a protective immunological response. With this technique, however, comes potential problems, including the possibility of insertional mutagenesis, which could lead to the activation of oncogenes or the inhibition of tumor suppressor genes source
So what scientific evidence is there of DNA/SV40 promoter contamination?
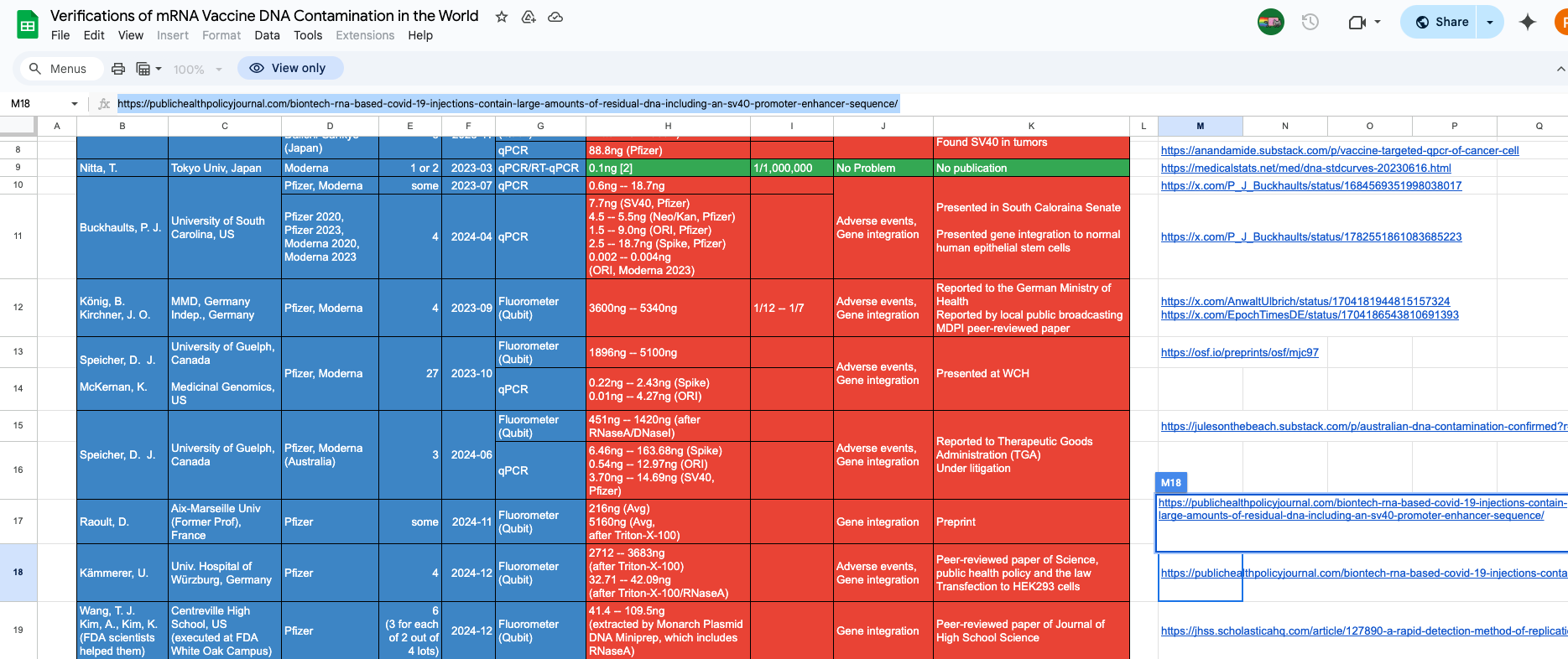
Turns out quite a few papers have replicated the DNA and SV40 contamination. Here is a google doc of the advances so far:
Let us begin:
Background: BNT162b2 RNA-based COVID-19 injections are specified to transfect human cells to efficiently produce spike proteins for an immune response.
Methods: We analyzed four German BNT162b2 lots applying HEK293 cell culture, immunohistochemistry, ELISA, PCR, and mass spectrometry.
Results: We demonstrate successful transfection of nucleoside-modified mRNA (modRNA) biologicals into HEK293 cells and show robust levels of spike proteins over several days of cell culture. Secretion into cell supernatants occurred predominantly via extracellular vesicles enriched for exosome markers. We further analyzed RNA and DNA contents of these vials and identified large amounts of DNA after RNase A digestion in all lots with concentrations ranging from 32.7 ng to 43.4 ng per clinical dose. This far exceeds the maximal acceptable concentration of 10 ng per clinical dose that has been set by international regulatory authorities. Gene analyses with selected PCR primer pairs proved that residual DNA represents not only fragments of the DNA matrices coding for the spike gene, but all genes from the plasmid including the SV40 promoter/enhancer and the antibiotic resistance gene.
Conclusion: Our results raise grave concerns regarding the safety of the BNT162b2 vaccine and call for an immediate halt of all RNA biologicals unless these concerns can be dispelled.

Conclusion: These data demonstrate the presence of billions to hundreds of billions of DNA molecules per dose in these vaccines. Using fluorometry, all vaccines exceed the guidelines for residual DNA set by FDA and WHO of 10 ng/dose by 188 – 509-fold. However, qPCR residual DNA content in all vaccines were below these guidelines emphasizing the importance of methodological clarity and consistency when interpreting quantitative guidelines. The preliminary evidence of a dose-response effect of residual DNA measured with qPCR and SAEs warrant confirmation and further investigation. Our findings extend existing concerns about vaccine safety and call into question the relevance of guidelines conceived before the introduction of efficient transfection using LNPs. With several obvious limitations, we urge that our work is replicated under forensic conditions and that guidelines be revised to account for highly efficient DNA transfection and cumulative dosing

In this study, residual DNA was detected from six vials of two different lots of Pfizer COVID-19 mRNA vaccines. The estimated amount of residual DNA in one human dose appears to be 6 to 470 times 10 ng.
This study was performed at the FDA white oak campus with their assistance. Literal high school students can and did perform this work. The regulatory agencies are incompetent for not doing it themselves.
Again DNA getting transfected into a cell by any means can result in cancer.

And the DNA plasmids appear to transmissible:
IMPORTANCE Asymptomatic laboratory workers who tested positive for SARS-CoV-2 for days to months were found to harbor a laboratory plasmid vector containing SARS-CoV-2 DNA, which they had worked with in the past, in their nasal secretions. While prior studies have documented contamination of research personnel with PCR amplicons, our observation is novel, as these individuals shed the laboratory plasmid over days to months, including during isolation in their homes. This suggests that the plasmid was in their nasal tissues or that bacteria containing the plasmid had colonized their noses. While plasmids are generally safe, our detection of plasmid DNA in the nasal secretions of laboratory workers for weeks after they had stopped working with the plasmid shows the potential for these reagents to interfere with clinical tests and emphasizes that occupational exposures in the preceding months should be considered when interpreting diagnostic clinical tests. Source
There are more.


Dr. Peter Kotlar 🇸🇰 explains that in every single tested vial there is an enormous amount of DNA in some cases more than mRNA.

This is from Dr. Jessica Rose “Expert Report for Charles Hoffe”. A dose response for reports of cancer.
On to gene “therapy”.

So gene therapy has potential cancer risks. Got it.
I could provide endless references SV40 is openly used in gene therapy. So are the covid quackines gene therapy?
One critical starting material for mRNA manufacturing is the DNA template encoding the antigen [15]. At Pfizer, we utilized prior plasmid DNA (pDNA) manufacturing technology expertize from Pfizer’s Gene Therapy Program.
Oh. So pfizer admit it took its DNA plasmid from its Gene Therapy program
Currently, mRNA is considered a gene therapy product by the FDA. Unlike certain gene therapies that irreversibly alter cell DNA and could act as a source of side effects, mRNA-based medicines are designed to not irreversibly change cell DNA; however, side effects observed in gene therapy could negatively impact the perception of mRNA medicines despite the differences in mechanism. In addition, because no product in which mRNA is the primary active ingredient has been approved, the regulatory pathway for approval is uncertain. The number and design of the clinical trials and preclinical studies required for the approval of these types of medicines have not been established, may be different from those required for gene therapy products, or may require safety testing like gene therapy products
And what is the definition of Gene Therapy?
Gene therapy is a technique that uses a gene(s) to treat, prevent or cure a disease or medical disorder. Often, gene therapy works by adding new copies of a gene that is broken, or by replacing a defective or missing gene in a patient's cells with a healthy version of that gene. source
As the modified mRNA is not adding new copies of a gene that is broken, missing or defective and is instead providing the code for cardiogenic spike protein is not a healthy versionit is not “therapy”. It is just gene destroying.
Hematologic cancer developed in 7 of 67 patients after the receipt of eli-cel
so 10.4% of gene therapy patients got a blood cancer…yes the DNA plasmid that grew this product has an SV40 promoter / origin of replication ori. Credit to Sasha Latypova for the find.
Hematologic cancer developed in a subgroup of patients who were treated with eli-cel; the cases are associated with clonal vector insertions within oncogenes and clonal evolution with acquisition of somatic genetic defects
So it results in blood cancer. Did this happen after the Covid-19 quacksines? You bet it did.
Lymphoma / Leukemia Case Serious and Systematic Review

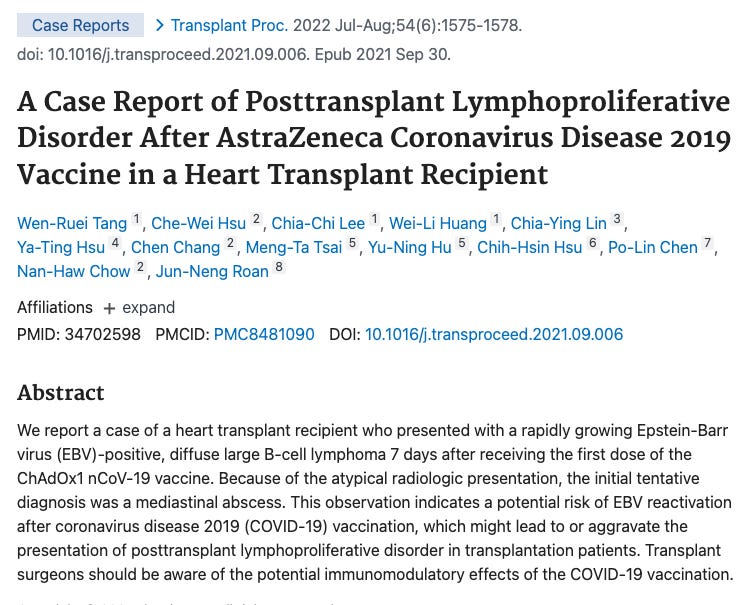
“This systematic review comprehensively analyzes cases of lymphoma occurring after COVID-19 vaccination and underscores the potential risks associated with COVID-19 vaccination. We found that lymphoma secondary to SARS-CoV-2 vaccination primarily presents as lymphadenopathy, with some patients experiencing lymph node pain, fatigue, and swelling at the injection site. The affected population is predominantly female and elderly individuals. Furthermore, the occurrence of lymphoma is associated with the type of SARS-CoV-2 vaccine, primarily mRNA vaccines. However, further research is needed to elucidate the potential interplay and mechanisms underlying the relationship between COVID-19 vaccines and lymphoma.” source
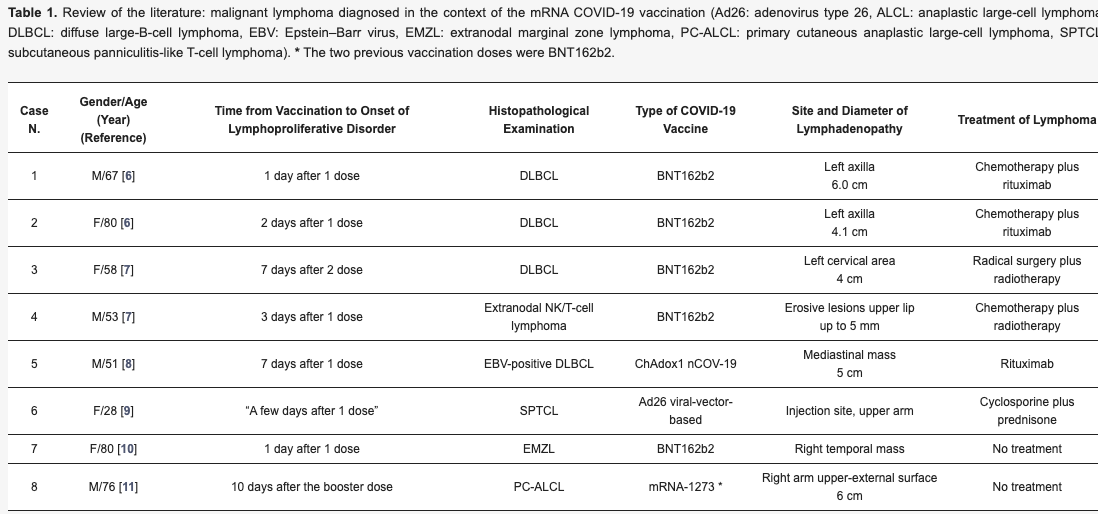
There are many case studies showing it is not a theoretical concern. It is happening to real patients. The reference section has a good collection:
Arens AIJ, Hebeda KM, Hutchings M, et al. Axillary lymph nodes on PET in Hodgkin lymphoma after COVID-19 vaccination [J]. EJHaem. 2021 Nov;2(4):885-886.
Mizutani M, Mitsui H, Amano T, et al. Two cases of axillary lymphadenopathy diagnosed as diffuse large B-cell lymphoma developed shortly after BNT162b2 COVID-19 vaccination [J]. J Eur Acad Dermatol Venereol. 2022 Aug;36(8):e613-e615.
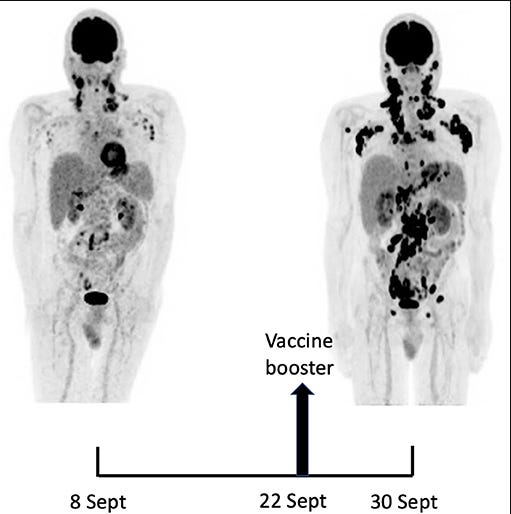
Cavanna L, Grassi SO, Ruffini L, et al. Non-Hodgkin Lymphoma Developed Shortly after mRNA COVID-19 Vaccination: Report of a Case and Review of the Literature [J]. Medicina (Kaunas). 2023 Jan 12;59(1):157.
Zamfir MA, Moraru L, Dobrea C, et al. Hematologic Malignancies Diagnosed in the Context of the mRNA COVID-19 Vaccination Campaign: A Report of Two Cases [J]. Medicina (Kaunas). 2022 Jun 30;58(7):874.
Hobayan CG, Chung CG. Indolent cutaneous lymphoma with gamma/delta expression after COVID-19 vaccination [J]. JAAD Case Rep. 2023 Feb;32:74-76.
Bresler SC, Menge TD, Tejasvi T, et al. Two cases of challenging cutaneous lymphoid infiltrates presenting in the context of COVID-19 vaccination: A reactive lymphomatoid papulosis-like eruption and a bona fide lymphoma [J]. J Cutan Pathol. 2023 Mar;50(3):213-219.
Tachita T, Takahata T, Yamashita S, et al. Newly diagnosed extranodal NK/T-cell lymphoma, nasal type, at the injected left arm after BNT162b2 mRNA COVID-19 vaccination [J]. Int J Hematol. 2023 Oct;118(4):503-507.
Kreher MA, Ahn J, Werbel T, et al. Subcutaneous panniculitis-like T-cell lymphoma after COVID-19 vaccination [J]. JAAD Case Rep. 2022 Oct;28:18-20.
Revenga-Porcel L, Peñate Y, Granados-Pacheco F. Anaplastic large cell lymphoma at the SARS-CoV2 vaccine injection site [J]. J Eur Acad Dermatol Venereol. 2023 Jan;37(1):e32-e34. Figer1 Data retrieval and screening process Table1 Basic information for lymphoma patients
I will highlight some and add new ones.
Dont you find it startling people are getting lymphoma days after vaccination? Usually it would take years of poor lifestyle choices like smoking to cause cancer.

Pfizer/BioNTech (BNT162b2) is a messenger RNA (mRNA) vaccine that is highly effective in preventing the most severe outcomes of COVID-19 infection. Nucleoside-modified severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) mRNA vaccines induce effective stimulation of T follicular helper (TFH) cells, leading to a robust germinal center B cell response. Side effects from the BNT162b2 vaccination, including significant lymphadenopathy, have been reported previously. Here, we present a case of angioimmunoblastic lymphoma (AITL), a rare, peripheral T-cell lymphoma with RHOA-G17v-mutated gene developing in a patient following BNT162B2 vaccine with a plausible explanation. A 60-year-old Asian female received her first dose of Pfizer BNT162B2 mRNA vaccine in August 2021. Right after her vaccination, she developed right axillary lymphadenopathy. She received her second vaccine dose in September 2021. Thereafter, she developed lymph node (LN) enlargement in her neck and groin. She underwent left posterior cervical and left groin LN excisional biopsy in April 2022 due to persistent palpable lymphadenopathy. Biopsy results then demonstrated benign follicular hyperplasia. For progressive B symptoms, a right axillary LN biopsy was done, which demonstrated AITL, with molecular studies revealing mutation in TET-2, IDH-2, and RHOA-G17v genes. Progression of AITL following BNT162B2 mRNA vaccine is limited in literature. Our case demonstrates a plausible correlation between the diagnosis of AITL following mRNA vaccination due to the malignant transformation of the TFH cells in patients who have a predisposing mutation of RHOA-17v. Given the rarity of AITL and the heterogeneity of molecular findings, more studies are needed to establish such an association. source
This patient was positive for EBV as well if you read the full text.
Notice how they are mentioning the latent EBV being reactivated by the quacksines? I remember this from the Yale Long Post- Vaccination paper.
a small fraction of the population reports a chronic debilitating condition after COVID-19 vaccination, often referred to as post- vaccination syndrome (PVS). To explore potential pathobiological features associated with PVS, we conducted a decentralized, cross-sectional study involving 42 PVS participants and 22 healthy controls enrolled in the Yale LISTEN study. Compared with controls, PVS participants exhibited differences in immune profiles, including reduced circulating memory and effector CD4 T cells (type 1 and type 2) and an increase in TNFα+ CD8 T cells. PVS participants also had lower anti-spike antibody titers, primarily due to fewer vaccine doses. Serological evidence of recent Epstein-Barr virus (EBV) reactivation was observed more frequently in PVS participants. Further, individuals with PVS exhibited elevated levels of circulating spike protein compared to healthy controls.
Oh. Just like it reactivates shingles it also reactivates the cancer causing EBV. They also had immunosuppression as measured by reduced T cells and elevated spike protein concentrations (a potentially cancer inducing protein see S2 and P53).
positive for EBV.
They are warning if you get swelling of your lymph nodes it could be a sign of malignancy.
Isn’t this a complication of (V)AIDS? yeah lowered T cell count and immunosuppression like I mentioned. I wont even bring up the HIV inserts like GP120.
This one is for AZ which uses adenovirus (monkey virus) as a vector but again EBV reactivation.

The overall SIR estimates suggested an increased risk of overall cancer in IgG4-RD patients (SIR 2.57 95% CI 1.72–3.84) compared with the general population. The specific SIRs for pancreas and lymphoma were higher than those of the general population in IgG4-RD patients (SIR 4.07 95% CI 1.04–15.92, SIR 69.17 95% CI 3.91–1223.04, respectively)…Compared with the general population, patients with IgG4-RD appear to have a higher risk of overall cancer, especially pancreatic and lymphoma. The risk of lung and gastric cancer was not different between IgG4-RD patients and the general population. source
a 69 times risk for lymphoma with IgG4 RD. We know multiple injections causes IgG4 to raise from near 0% to 20% of total antibodies.
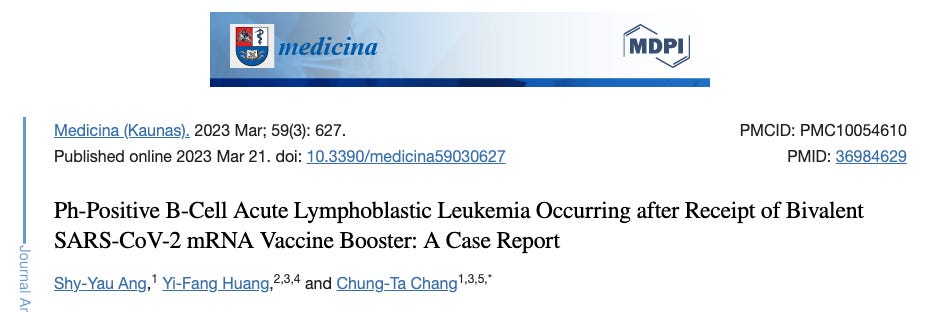
We reported the first case of Ph-positive B-cell acute lymphoblastic leukemia (ALL) occurring after a bivalent mRNA COVID-19 vaccine inoculation. The otherwise healthy 43-year-old female patient had a total of six spike antigen exposures in the past 1.5 years. Informative pre-vaccine tests and bone marrow study results were provided. Although the causal relationship between bivalent vaccinations and the subsequent development of Ph–positive B-cell ALL cannot be determined in the case report, we propose that anti-spike protein immune responses could be a trigger for leukemia. Clinicians must investigate the hematopoietic adverse events closely after COVID-19 vaccinations. Further pre-clinical studies to investigate the safety of bivalent mRNA COVID-19 vaccine are required
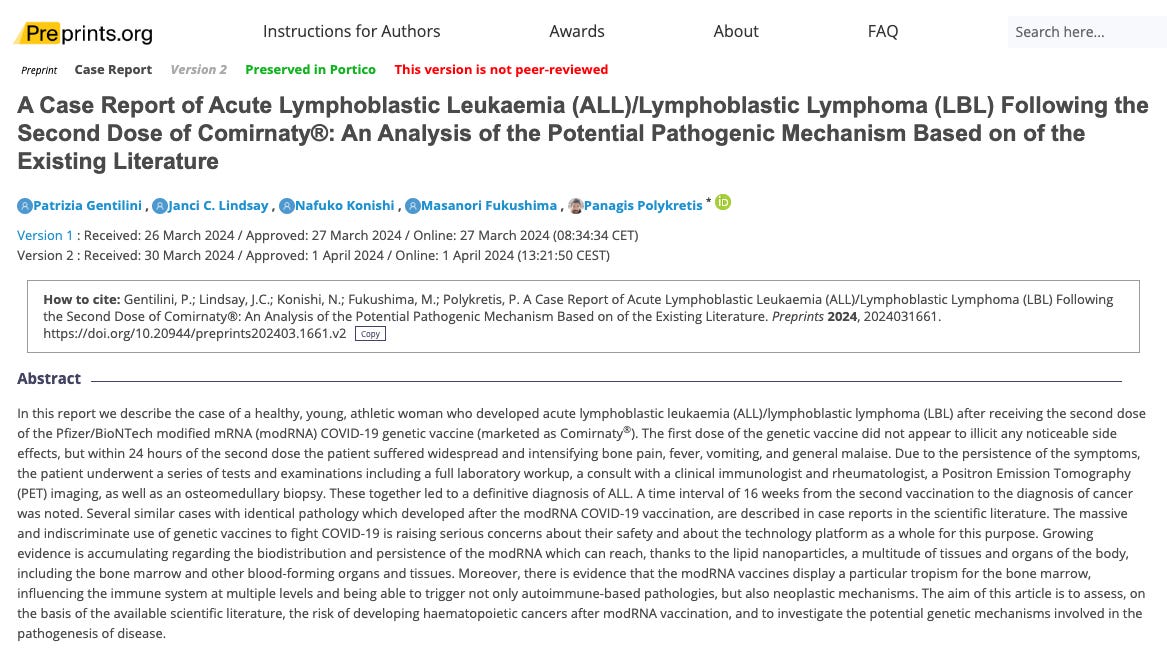
This paper does an excellent job with plausible mechanisms:
Potential Carcinogenic Mechanisms Induced by COVID-19 modRNA Vaccines
Several mechanisms have been proposed by which the current modRNA COVID-19 vaccines may exert a carcinogenic effect, inducing both de novo tumour formation and the recurrence of neoplastic diseases in remission. It is also evident, that the genetic material and the vaccine derived spike protein have a significant impact on the immune system and may compromise immune surveillance against altered cellular clones in a manner that could lead to cancer.
The main alterations induced by modRNA COVID-19 vaccines reported in literature, that may have an oncogenic outcome are listed below:
(i)
The alteration of the inhibitory immune checkpoint mediated by the programmed cell death protein 1 (PD-1, CD279), which is primarily found on T-cells, mature B-cells, and other immune cells. The overexpression of the programmed death-ligand 1 (PD-L1), observed in vaccinated individuals, leads to T-cell immunosuppression, impairing cancer surveillance [54].
(ii)
The interaction between the S2 subunit of the spike protein and the oncosuppressor proteins p53, BRCA1, and BRCA2, which regulate downstream genes in response to numerous cellular stress and play a crucial role in preventing cancer [55].
(iii)
The impairment in type I interferon (IFN) signalling, which play essential roles in inflammation, immunomodulation, tumour cell recognition, and T-cell responses [56]. Differential gene expression analysis of peripheral dendritic cells revealed dramatic upregulation of type I and type II IFNs in COVID-19 patients, but not in vaccinees. All this supports the possibility that COVID-19 genetic vaccines actively suppress the production of type I IFN which play a fundamental role in the immune reaction in response to multiple stressors, especially viral infections and tumours. In the presence of a viral infection, the production of type I IFN drastically increases and IFN-α, released in the lymph nodes, induces B-cells to differentiate into plasmablasts and subsequently, thanks to IL6, to evolve into antibody-secreting plasma cells. As regards the anti-tumour action of IFNs, this occurs through both direct and indirect mechanisms. Direct effects include cell cycle arrest, induction of cell differentiation, initiation of apoptosis, and activation of natural killer and CD8+ T-cells. The indirect anti-tumour effects are mainly due to the activation of transcription factors which improve the expression of at least 150 genes also involved in apoptosis.
(iv)
Increased Transforming Growth Factor Beta (TGF-β) Production. The interaction between the SARS-CoV-2 spike protein and the angiotensin-converting enzyme 2 (ACE2) induces TGF-β release by cells such as alveolar and tissue macrophages, lung epithelial cells, endothelial cells and B lymphocytes, promoting epithelial-mesenchymal transition (EMT) [57]. This process could explain the particular rapidity of onset and evolution of tumour forms arising following the administration of the COVID-19 genetic vaccines. In fact, the TGF-β is a growth factor capable of inducing in already differentiated cells a “regression” towards the mesenchymal state (a state typical of the early stages of embryonic life), with the ability to metastasize and greater biological aggressiveness.
(v)
The presence of LNP-encapsulated DNA contamination originating from residual plasmid DNA from DNA plasmids used during the manufacturing process of the Pfizer/BioNTech and Moderna modRNA genetic vaccines [58,59]. The residual DNA detected in the modRNA genetic vaccines is high in copy number and contains elements such as: functional promoters, open reading frames (ORFs), origins of replication and nuclear targeting sequences [59]. In the case of the Pfizer/BioNTech genetic vaccine, such plasmids have been engineered with a mammalian SV40 promoter-enhancer-ori from the oncogenic virus Simian Virus 40 (SV40) along with a nuclear targeting sequence (NTS) [58,59]. This human compatible promoter is not required for the expression of these plasmids in the E. coli bacterial expression system and its presence is highly unusual as it poses a significant oncogenic risk that is not needed for the plasmid’s stated purpose. The FDA has guidance for plasmid DNA-based genetic vaccines and while the modRNA are not defined as DNA based-vaccines, the contaminating plasmids’ design is consistent with this application and it is expected that portions of the contaminating plasmid DNA with eukaryotic promoters and enhancers will pose the same risks of insertional mutagenesis. FDA advises the following: “Plasmid biodistribution, persistence and integration studies were initially recommended to examine whether subjects in DNA vaccine trials were at heightened risk from the long-term expression of the encoded antigen, either at the site of injection or an ectopic site, and/or plasmid integration. Theoretical concerns regarding DNA integration include the risk of tumorigenisis if insertion reduces the activity of a tumor suppressor or increases the activity of an oncogene. In addition, DNA integration may result in chromosomal instability through the induction of chromosomal breaks or rearrangements.” [60]. Additionally, the presence of the contaminating plasmids is far above the regulated limits for naked DNA contamination on vaccines [58,59]. As recently reported by Cancer Geneticist Prof. Buckhaults [61] and by Toxicologist and Molecular Biologist Janci Lindsay, Ph.D. [62] before the South Carolina Senate Medical Affairs Ad-Hoc Committee, these are extremely serious and unexplainable contaminants of the Pfizer/BioNTech modRNA vaccines, because they increase the likelihood that these contaminating sequences from this oncogenic virus as well as other sequences contained within the plasmids and encapsulated within the LNPs, will integrate into the DNA of the vaccinees with consequences that are difficult to predict. Insertional mutagenesis is often leading to cancer, and in fact, gene therapy has long been known to bear an oncogenic risk as recognized by the FDA in their guidance on plasmid DNA vaccines [60], and the previous studies cited [23,24,25]. According to Buckhaults, the urgency of the pandemic crisis induced the pharmaceutical companies to take some “shortcuts”, using bacteria for the mass production of the modRNA vaccines. The SV40 DNA sequences derive from a plasmid engineered for the modRNA production in bacteria, specifically modified to include the SPIKE gene. Pfizer/BioNTech tried to solve the problem by adding the enzyme deoxyribonuclease to chop the plasmid into millions of small fragments. However, according to Prof. Buckhaults, this actually increased the risks because the more fragments there are, the more likely it is that one of them will fit into the genome and interfere with crucial genes. Prof. Buckhaults and Dr. Lindsay expressed their concern about the theoretical, but very real risk of future cancer in some people, depending on where foreign pieces of DNA integrate in the genome, potentially disrupting suppressor genes or activating oncogenes. In fact, as relayed earlier the SV40 virus is a known oncogenic virus when intact [63,64]. There is also the additional potential for the modRNA to be reverse transcribed to DNA through the reverse transcriptase activity of LINE-1, as previously demonstrated by Aldén et al., especially in tissues such as the testes and ovaries as well as the bone marrow that are rich in this transcription factor [59,65].
(vi)
The role of the immunoglobulin subtype IgG4 in cancer immune evasion. Wang et al. found that IgG4-containing B lymphocytes and IgG4 concentration were significantly increased in cancer tissues, as well as in the serum of patients with cancer [66]. Both were positively correlated with worse prognoses and increased cancer malignancy. Previous works reported that IgG4 was generated locally in melanoma, playing an important role in removing the tumour from the control of the immune system and therefore facilitating its development [67,68]. Increased production of IgG4 is normally associated with prolonged exposure to antigens, and their interaction with antibodies of the IgG and IgE classes through their Fc domains has been reported [69]. IgG4 is in fact endowed with a dual role, as it can suppress or stop inflammation by competing with inflammatory IgE for binding to the antigen, in the case of allergies and infections from helminths and filarial parasites or, on the contrary, IgG4 can lead to serious autoimmune [70] and tumour diseases, playing an essential role in the “immune evasion” of cancer cells. Recent studies indicate that repeated modRNA vaccinations against COVID-19 shift the antibody response towards the IgG4 subclass with a decrease in FcγR-dependent effector activity and an increased mortality in case of COVID-19 infection [71,72,73]. In cohorts of healthy healthcare workers, it was demonstrated that several months after the second dose the SARS-CoV-2-specific antibodies were increasingly composed of non-inflammatory IgG4, which were further enhanced by a third modRNA vaccination and/or by infections of SARS-CoV-2 variants [72]. IgG4 antibodies, among all spike-specific IgG antibodies, increased on average from 0.04% shortly after the second vaccination, to almost 20% (19.27%) after the third vaccination [73]. In conclusion, the increase in IgG4 following repeated administration of modRNA vaccines is undoubted and this generates serious concerns regarding the involvement of IgG4 in the “immune evasion” of cancer cells.
(vii)
The incorporation of m1Ψ into the modRNA of the genetic vaccines causes ribosomal frame-shifting during translation, which can lead to the production of numerous peptide products that are expressed differently in each individual [29]. Given that these unidentified peptides may have unknown antigenic and auto-immune potential, they pose a serious risk for carcinogenesis that should be deeply investigated.
Conclusions
The development and widespread use of modRNA vaccines have raised significant concerns globally, leading to adverse events and complications in both healthy individuals and those with pre-existing conditions. Reports of increased cases of a variety of cancers [18], including highly aggressive cancers, termed “Turbo Cancer” [20] and the unexpected recurrence of cancers after decades of remission, have been independently noted by oncology experts and researchers worldwide, with several publications supporting these observations [35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]. Understanding the mechanisms behind the carcinogenic effects of the modRNA COVID-19 vaccines is crucial. Immune system alterations, notably T-cell suppression, the decreased production of IFN type I, interference with oncosuppressor genes and proteins, inhibition of DNA repair mechanisms, and overexpression of cell death proteins in T-cells, are key factors facilitating neoplastic/oncogenic transformation [54,55,56]. Increased TGF-β production, promoting EMT, may explain the aggressive nature of observed tumours [57]. Additionally, the detection of hazardous and unexplainable contamination of the modRNA vaccines with plasmid DNA sequences deriving from the manufacturing process needs to be investigated. What is the purpose for the addition of a mammalian promoter and nuclear targeting sequence from the SV40 oncovirus in the plasmid used in the manufacturing process of the Pfizer/BioNTech genetic vaccine, supposedly meant to only be used to grow copies in bacteria, where a mammalian promoter and obviously a nuclear targeting sequence, is not needed? Such very concerning issues must be appropriately addressed by the global safety and regulatory agencies. Just as the risk of developing myocarditis and pericarditis following modRNA COVID-19 vaccination has been recently acknowledged [74], similar attention should be paid to assess the potential risk of developing cancer associated the with the genetic vaccines. Since the development of modRNA vaccines is also already in motion for other diseases and this platform is planned to replace the existing traditional vaccine platform for the childhood vaccines, the carcinogenic risk of these technologies, which has been long known to the gene therapy platform, especially for leukaemias and lymphomas, represents a field of research that cannot be ignored, given that the fundamental principle of medicine, which is “primum non nocere”. It is therefore crucial to perform extensive pharmacodynamic, pharmacokinetic and genotoxicity evaluations, as well as population-based observational studies, in order to assess the potential carcinogenic risk posed by the genetic vaccines and to understand its pathogenic mechanism.

This paper remind me of the Hematological cancers after gene therapy paper. Who knew? I did.
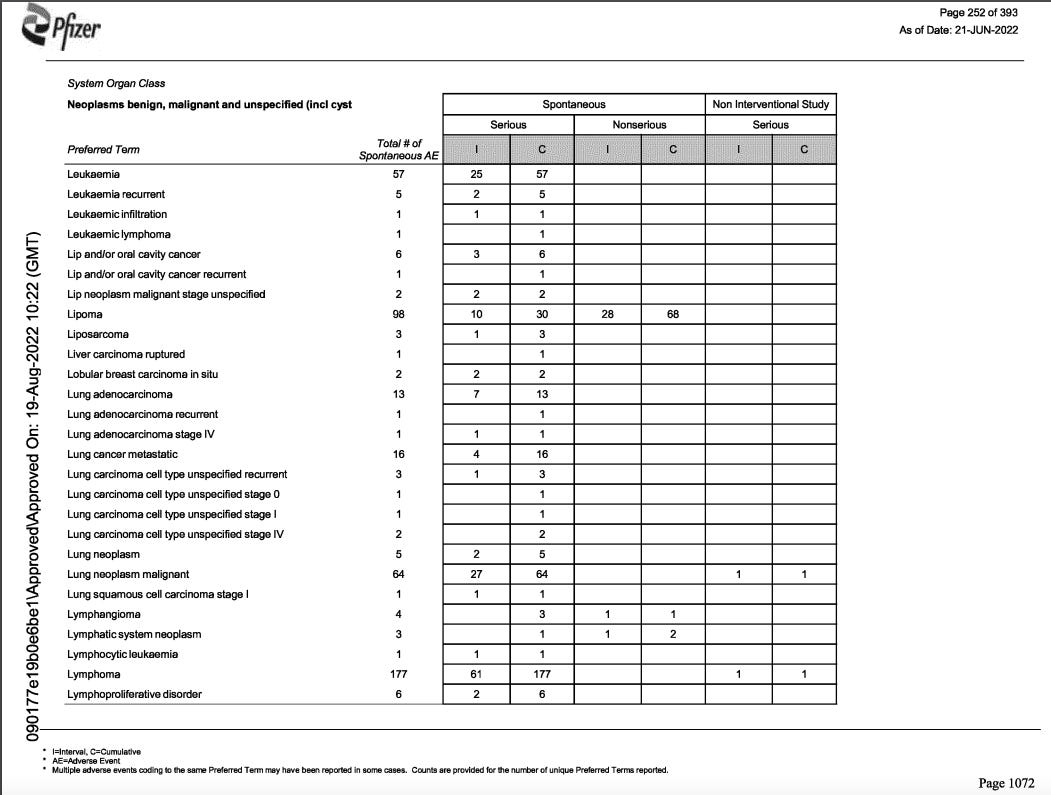
Pfizer also knew it was causing blood cancers and had 3711 reports of cancer after their product. source
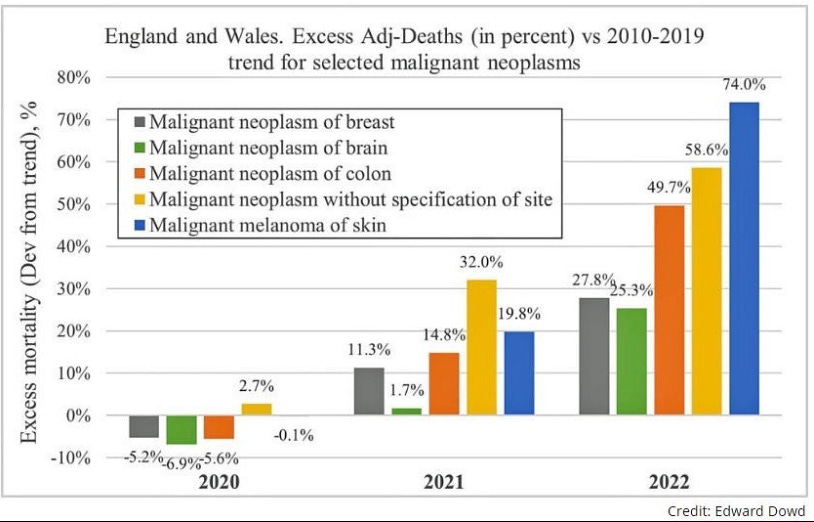
So are cancer rates rising after the roll out? Yes.


Dr. Baffled cant figure it out but I can.
Lets add in some populations studies to strengthen our causation argument. This one is from the the US.
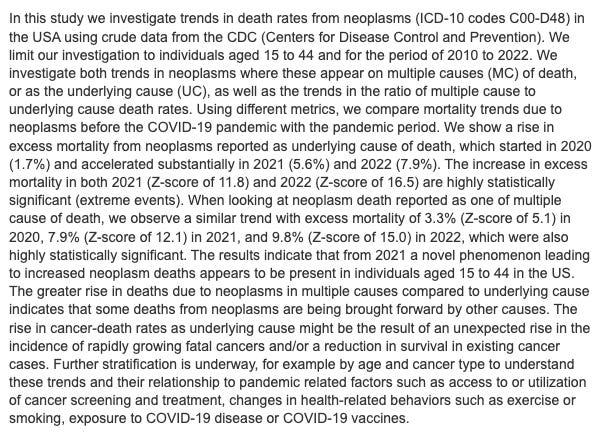
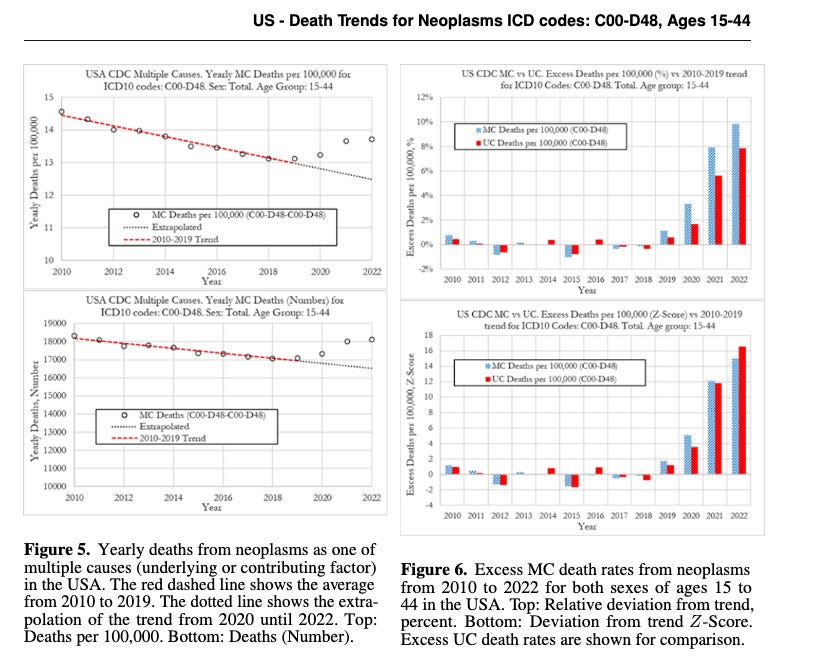
When analyzing UC death rates from neoplasms,our computations show that the excess death rates from neoplasms for the 15-44 age group were 1.7% in 2020, 5.6% in 2021, and 7.9% in 2022 (Figure 4). Even though the deviation from trend was small, the excess death rate in 2020 was statistically significant with a Z-score of 3.5. The excess UC death rates in 2021 and 2022 can be considered extreme eventswith respective Z-scores of 11.8 and 16.5
The next source is so retracted and heavily censored it only has a “Tombstone” source

Luckily I downloaded and saved it:
It is an update from a previously peer-reviewed and published in Cureus. It was retracted without discussion.

Statistically significant increases in age-adjusted mortality rates of all cancer and some specific types of cancer, namely, ovarian cancer, leukemia, prostate, lip/oral/pharyngeal, pancreatic, and breast cancers, were observed in 2022 after two-thirds of the Japanese population had received the third or later dose of SARS-CoV-2 mRNA-LNP vaccine. These particularly marked increases in mortality rates of these ERα-sensitive cancers may be attributable to several mechanisms of the mRNA-LNP vaccination rather than COVID-19 infection itself or reduced cancer care due to the lockdown. The significance of this possibility warrants further studies. source
Oh. Okay then. All pro-vaxx papers make absurd conclusions like “benefits outweigh risk” and “saved millions of lives” and their methods of estimation and surrogate outcomes are not “proven with the data presented” so lets retract them all.
Here are some highlights from the version that was just fully deleted from the pre-print server with no justification.
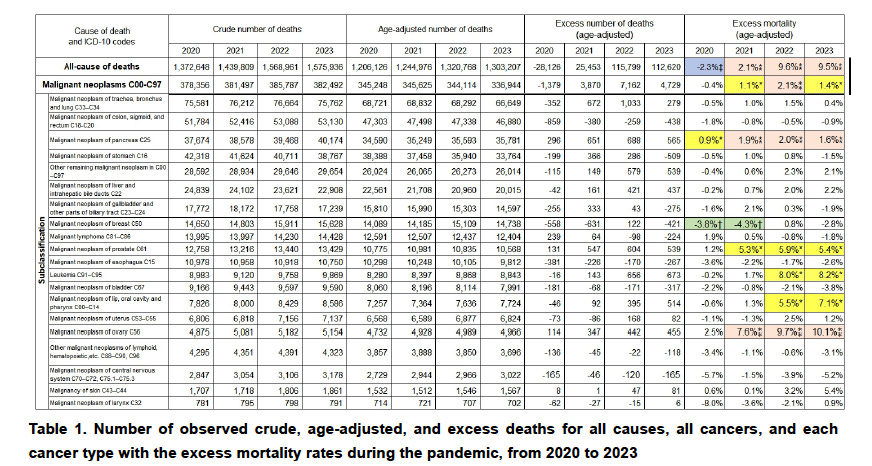
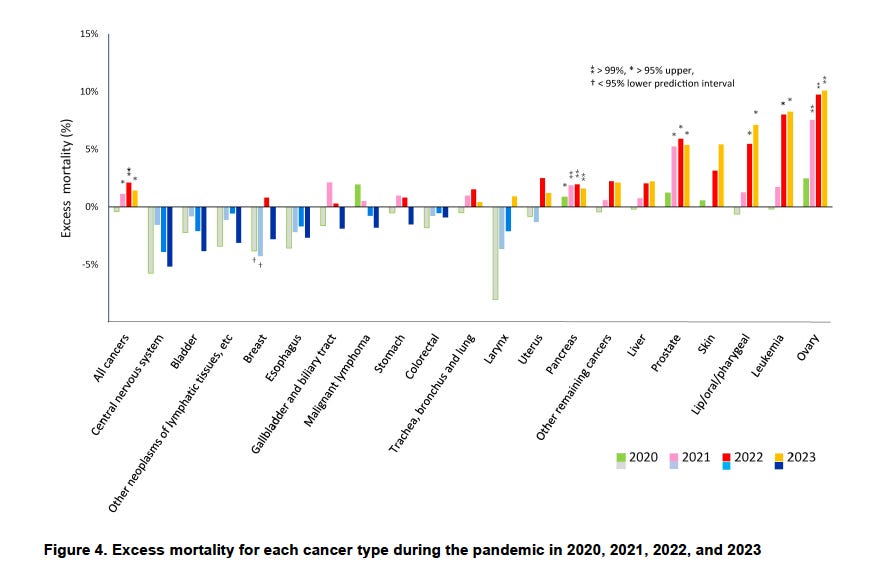
Its a bit surprising lymphoma was not found in this data set but leukemia was and follows the general trend of a 7-10% increase in certain types of cancer since the roll out. I think I will stop there.
Summary:
SV40 was found in the polio vaccines in the 1950s. Instead of stop using the monkey kidney cells they came from they deliberately made a new cell line from them (VERO) and deliberately chose SV40 in gene therapy for its ability to target the nucleus. It causes blood cancer in the gene therapy patients and it is causing turbo cancers in those that injected SV40 promoters in the covid injection and others including hep B and influenza without their knowledge. It also reactivates other cancer causing viruses like EBV. The DNA alone which even exceeds the mRNA content in some vials can cause cancer. This was known for decades and was deliberate done most likely to reduce the population and sell expensive and ineffective cancer drugs that also cause hyperprogressive disease/turbo cancer (Im looking at you Merck / Keytruda/ PDL1 and obviously Pfizer and BioNtech as well)
The craziest story ever told. How humanities addiction and blind faith in “safe and effective” quacksines lead to an increasingly unmanageable cancer epidemic. You should want all vials confiscated and tested for DNA and SV40 sequences. It is not contamination when it is deliberate. All cancer biopsies should be tested in the same way to confirm what we already know. The SV40 that was concealed from the public is integrating into cancer cells.
This SV40 / DNA issue is just one of the over 30 reasons I have provided from the scientific literature of why they are increasing the rate of turbo cancer. See my other 3 substacks on this topic for elaboration.
Kudos to Dr. William Makis who has done great work creating awareness of this issue.
Thank you for your thorough research and piecing altogether into a readable report. Most appreciate you educating the reader.
This research casts light on the dangers of injecting pregnant women.
Amyloidogenic Fibrin Microclotting Following Prenatal mRNA Vaccination Exposure
https://kevinwmccairnphd282302.substack.com/p/amyloidogenic-fibrin-microclotting
We report the presence of amyloidogenic fibrils in the peripheral blood of a three-year-old child with documented in-utero exposure to maternal mRNA-based SARS-CoV-2 vaccination.
https://kevinwmccairnphd282302.substack.com/p/amyloidogenic-fibrils-in-a-post-gestational