“Extraordinary claims require extraordinary evidence.” Carl Sagan
Did Operation Warp Speed really save hundreds of millions of lives like Trump said? Believe it or not evidence is required for claims of benefit as well. Before we begin ponder this. Is it better for the public to be overestimating claims of benefit and minimizing claims of harm? I would argue claims of benefit should be subjected to the highest standards of evidence while claims of harm should be subjected to the precautionary principle to prevent damaging the public for a theoretical or exaggerated benefit. Despite my pseudonym I actually like science and wish more people would apply its principles.
There are no shortages of extraordinary fairytales in the fantasy world of vaccinology. I do not worship vaccines so I am not going to accept claims from their doctor-priests as a matter of faith. The word “vaccine” contains no magical meaning to me. It is derived from the latin word “vacca” for cow. This is appropriate as it is their sacred cash cow and many vaccines contain disgusting ingredients from cows including bovine casein, calf serum and albumin. Historically cowpox pus was added to the smallpox inoculation so this is likely the true reason for their being called “vaccines”. They really do consider you a pharm-animal, hence the fictional concept of “herd immunity” which is without empirical substantiation. I do not wish to be part of that kind of herd as the Lancet says.
I reject the unethical use of the magical spell “immunization”. Not a single injection on the schedule can provide sterilizing immunity, prevent transmission or provide herd immunity. They use the phrase “immunizations to prevent vaccine-preventable diseases” to induce the population into a trance-like belief that they provide immunity. This is a fraudulent and manipulative use of language to create belief in the product. I have tremendous examples of primary and secondary vaccine failure.
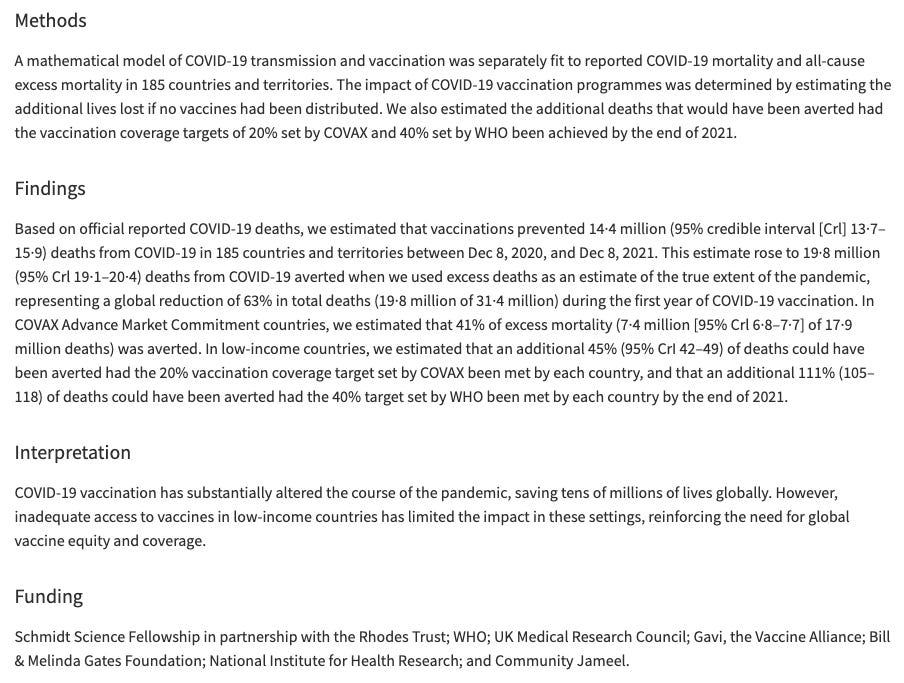
Most of the time even the so-called medical journals do not provide a citation when making their grandiose statements of worship. One of the most parroted claims is that vaccines saved hundred of millions of lives:
“We estimate 97 million deaths would be averted due to vaccination activities over 2000-2030 with 50 million deaths averted by activities between 2000 and 2019.” source
Do their methods satisfy evidence of causation for benefit?
“The beneficial effect of vaccination programmes cannot be assessed directly as the counterfactual, that is, the situation without vaccination, cannot be observed. Hence, models of disease risk and the impact of vaccination activities play a vital role in assessing the current burden”
WOW. No direct evidence. So a work of fiction then.
Note the extensive funding from Bill Gates/Gavi. I wonder what strings are attached for his funding on this lucrative liability-free investment.
“Estimates” are not part of science. This is just guessing and wishful thinking. They have even extended their findings into the future (2030) taking this into the realm of fortune telling. The methods describe using mathematical models. Where does they fit in on the medical evidence hierarchy?
I do NOT see math modelling studies anywhere. They are not considered evidence at all. Especially ones funded by Epstein’s friend Bill Gates. But he is dead, so I guess that doesn’t matter anymore.
Why does the bible of quacksinology have this medically untrained billionaire writing a foreword? He has no credibility. Forgive me if I think the motivation is for the 20:1 return on his investment and not the fraudulent claim of saving millions of lives.
Let me get back to the real science. Strictly speaking to make a credible claim that vaccines save lives you would need to use a high quality study/RCT where the primary end point is preventing death against the disease you are injecting against. You would also need an inert placebo group to compare it against. This is not done in a single licensure study with the exception of covid. Feel free to go look.
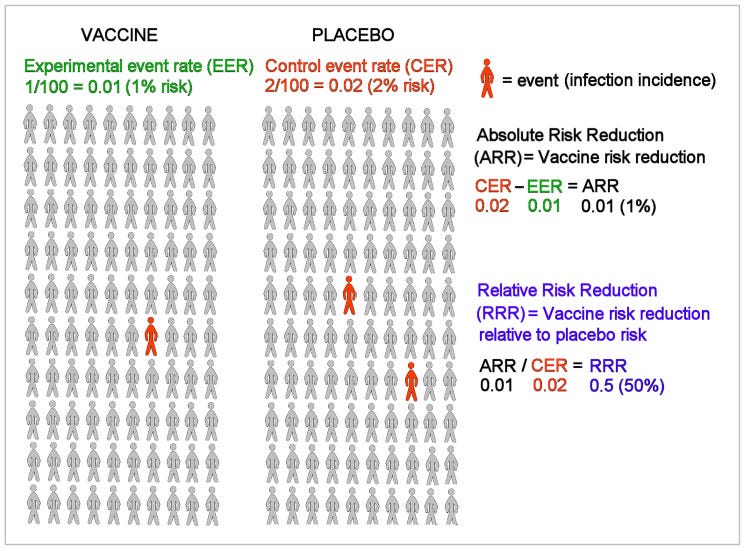
The Number Needed to Treat (NNT) is the average number of patients who need to be treated to prevent one additional bad outcome in our case death.
The number needed to treat is the inverse of the absolute risk reduction (ARR).
The ARR is the absolute difference in the rates of events between a given activity or treatment relative to a control activity or treatment, ie control event rate (CER) minus the experimental event rate (EER), or ARR = CER - EER.
NNTs are always rounded up to the nearest whole number and accompanied as standard by the 95% confidence interval2 .
Example: if a drug reduces the risk of a bad outcome from 50% to 40%, the ARR = 0.5 - 0.4 = 0.1. Therefore, the NNT = 1/ARR = 10.
The ideal number needed to treat would be 1 - ie all patients treated will benefit
Some points before I go further. One is that the studies always provide their efficacy in relative risk reduction (RRR) to make it sound more beneficial than it really is. They do this despite the FDA telling them to provide the absolute risk reduction (ARR). You cannot calculate the NNT without the ARR so this is critical information.
“Provide absolute risks, not just relative risks. Patients are unduly influenced when risk information is presented using a relative risk approach; this can result in suboptimal decisions. Thus, an absolute risk format should be used.” source
People made suboptimal decisions because of only being told the RRR. If the difference between absolute and risk reduction is not 100% clear to you yet do not feel bad. The doctors don’t understand it either or they would have told you the ARR for covid was less than 1% effective. Hopefully this clarifies.
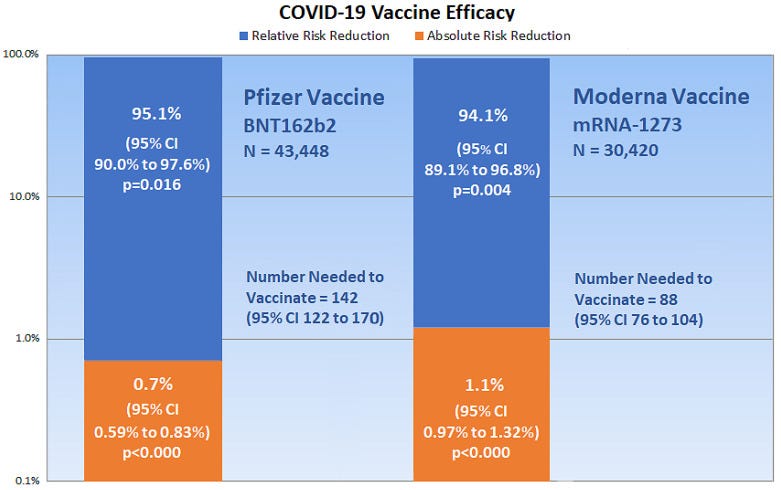
“Relative risk reduction and absolute risk reduction measures in the evaluation of clinical trial data are poorly understood by health professionals and the public. The absence of reported absolute risk reduction in COVID-19 vaccine clinical trials can lead to outcome reporting bias that affects the interpretation of vaccine efficacy. The present article uses clinical epidemiologic tools to critically appraise reports of efficacy in Pfzier/BioNTech and Moderna COVID-19 mRNA vaccine clinical trials. Based on data reported by the manufacturer for Pfzier/BioNTech vaccine BNT162b2, this critical appraisal shows: relative risk reduction, 95.1%; 95% CI, 90.0% to 97.6%; p = 0.016; absolute risk reduction, 0.7%; 95% CI, 0.59% to 0.83%; p < 0.000.”
The absolute risk reduction (ARR) in the RCT for the pfizer injection for preventing INFECTION (not death) was less than 1 percent (0.7%).
This puts the NNT to 142 to prevent a symptomatic case (and that is if you trust their highly fraudulent data which I do not ). But how many cases need to be prevented to prevent a death?
Even these authors provide information in relative risk. There is no beneficial effect on any mortality. The covid-19 specific mortality data was not statistically significant. The cardiovascular mortality was higher in the pfizer group. This is evidence of causation because of the dangerous mechanism of action, and strength of relationship.
“The analysis reported here is unique in that it is the first study of the original data from the Pfizer/BioNTech BNT162b2 mRNA vaccine clinical trial (CA4591001) to be carried out by a group unaffiliated with the trial sponsor. Our study is a forensic analysis of the 38 trial subjects who died between July 27, 2020, the start of Phase 2/3 of the clinical trial, and March 13, 2021, the data end date of their 6-Month Interim Report. Phase 2/3 of the trial involved 44,060 subjects who were equally distributed into two groups and received Dose 1 of either the BNT162b2 mRNA vaccinated or the Placebo control (0.9% normal saline). At Week 20, when the BNT162b2 mRNA vaccine received Emergency Use Authorization from the U.S. FDA, subjects in the placebo arm were given the option to be BNT162b2 vaccinated. All but a few accepted. Surprisingly, a comparison of the number of subject deaths per week during the 33 Weeks of this study found no significant difference between the number of deaths in the vaccinated versus placebo arms for the first 20 weeks of the trial, the placebo-controlled portion of the trial. After Week 20, as subjects in the Placebo were unblinded and vaccinated, deaths among this still unvaccinated cohort of this group slowed and eventually plateaued. Deaths in the BNT162b2 vaccinated subjects continued at the same rate. Our analysis revealed inconsistencies between the subject data listed in the 6-Month Interim Report and publications authored by Pfizer/BioNTech trial site administrators. Most importantly, we found evidence of an over 3.7-fold increase in number of deaths due to cardiovascular events in BNT162b2 vaccinated subjects compared to Placebo controls. This significant adverse event signal was not reported by Pfizer/BioNTech. Potential sources of these data inconsistencies are identified.” source
So that was the highest quality information available. No other prospective RCTs were conducted after the approval. Clearly there is no number to treat to prevent death.
How did it play out in the real-world data? Are there lower observational lines of evidence?Did it save lives or did all cause mortality increase? The BMJ admits excess mortality is high. This is not consistent with a life-saving intervention.
“ConclusionsExcess mortality has remained high in the Western World for three consecutive years, despite the implementation of containment measures and COVID-19 vaccines. This raises serious concerns. Government leaders and policymakers need to thoroughly investigate underlying causes of persistent excess mortality.” source
What about other countries like Germany. Were they saved by the life-saving quacksines?
“As is visible in Figure 8, the obvious hypothesis of a decrease in excess mortality with an increasing number of vaccinated persons is not correct. During periods when many persons were vaccinated, excess mortality seems to have increased more strongly compared to the same periods in the previous pandemic year. During the first and second vaccination periods in spring and summer 2021, an increase in cumulative excess mortality is observed, while the year before a decrease was observed. During the period of the third vaccination, parallel to the increase in vaccinations, an increase in cumulative excess mortality can be observed that starts earlier than in the year before. And in 2022, when large parts of the population have been vaccinated, the cumulative number of excess deaths showed a further increase, which even exceeds the previous pandemic year without vaccinations. There seem to be negative long-term effects either of the SARS-CoV-2 infections, COVID-19 measures, the COVID-19 vaccination, or most probably a combination of these” source
Oh! That looks kind of bad. Why are deaths not dropping like all those amazing historical vaccines.
Yes, very impressive declines in death before the vaccines were introduced. Glad these trends continued unlike the covid injection. I find it interesting when the vaccine cult believes observational data. Disease rates declined after the introduction of a vaccine. That is Causation!I am convinced. Just don’t show them the autism rates plotted against doses on the CDC schedule.
Being masters of fraud and deception look at what they tried to take credit for. Are you surprised they hid this behind a pay wall?
So are you giving credit to the vaccines when they were not available?
“Once again, nearly 90% of the decline in infectious disease mortality among US children occurred before 1940, when few antibiotics or vaccines were available” source
Even the authors of this Pediatrics paper thought it was important enough to repeat.
So is there any evidence at all it saved lives? Here is a pre-print done by a highly respected Stanford researcher John Ioannidis who famously provided the infection fatality rates of covid which were much lower than everyone was led to believe by the Imperial College of London who funded the study claiming vaccines saved millions of lives.
“The median IFR was 0.0003% at 0–19 years, 0.002% at 20–29 years, 0.011% at 30–39 years, 0.035% at 40–49 years, 0.123% at 50–59 years, and 0.506% at 60–69 years. IFR increases approximately 4 times every 10 years. Including data from another 9 countries with imputed age distribution of COVID-19 deaths yielded median IFR of 0.025–0.032% for 0–59 years and 0.063–0.082% for 0–69 years. Meta-regression analyses also suggested global IFR of 0.03% and 0.07%, respectively in these age groups. The current analysis suggests a much lower pre-vaccination IFR in non-elderly populations than previously suggested” source
Lets look deeper on what was required on its assumptions.
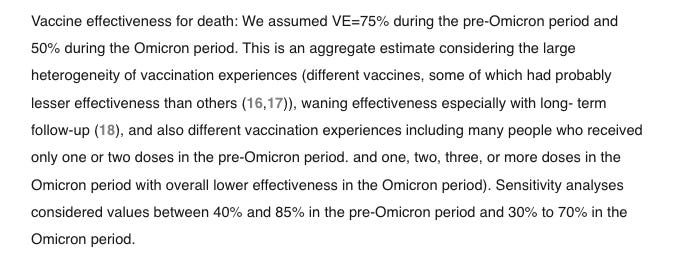
Over and over they say benefits exceed the risks. Well they refuse to even look at the risks. What about their assumptions for efficacy against death?
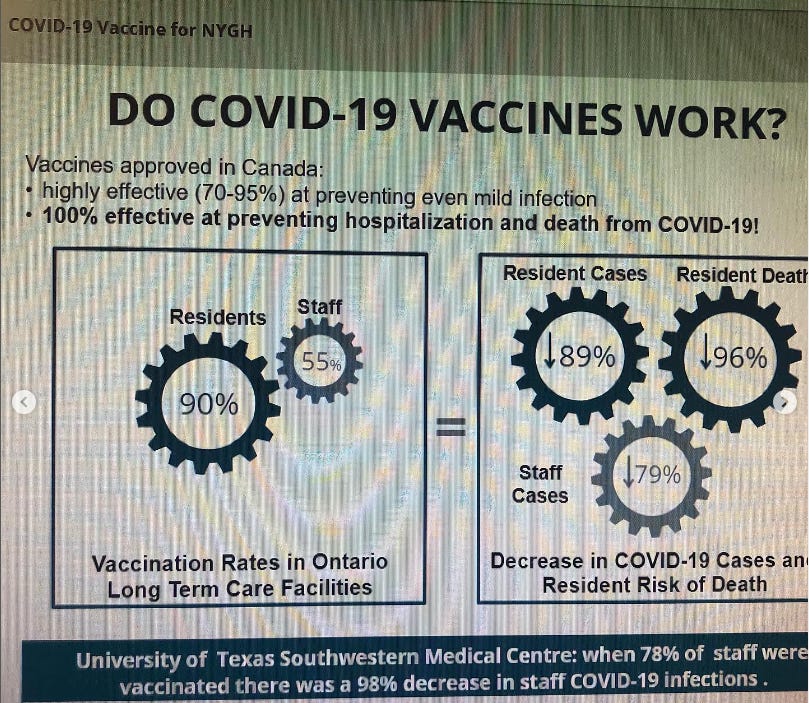
So they “assume” (very scientific) it is 75% effective against death. That is interesting because the informed consent course my wife had to take at North York General Hospital to keep her job said it was 100% effective against hospitalization and death. This was fraud and misrepresentation and coercion. No she did not take it and we suffered financially for her to avoid this DNA contaminated carcinogen.
Yeah 100% effective against death? Why are 10 times as many people dead in the injected cohort? source
I have many more studies of this type of conclusion:
“Among COVID-19 patients, mortality rate was significantly higher among Vax vs. NVax patients (p=0.002). The Charlson’s Comorbidity Index score (CCI) was also significantly higher among Vax vs. NVax COVID-19 patients. However, the mortality risk remained significantly higher (p=0.02) when we compared COVID-19 Vax vs. NVax patients with similar CCI score, suggesting that additional factors may increase risk of mortality. Higher levels of SARS-CoV-2 Abs were noted among survivors, suggestive of their protective role. We observed a trend for increased total IgG4 Ab, which promotes immune tolerance, in the Vax vs. NVax patients in week 3.
Conclusion: Although our cohort size is small, our results suggest that vaccination status of hospital-admitted COVID-19 patients may not be instructive in determining mortality risk. This may reflect that within the general population, those individuals at highest risk for COVID-19 mortality/immune failure are likely to be vaccinated. Importantly, the value of vaccination may be in preventing hospitalization as opposed to stratifying outcome among hospitalized patients, although our data do not address this possibility. Additional research to identify factors predictive of aberrant immunogenic responses to vaccination is warranted.” source
This is the estimates from the UK for preventing hospitalization. Pathetic. The number to treat should be close to 1. source
Back to our story. It cites references 16 and 17 as their basis for 75% effective against mortality. Let us look.
This is reference 16. source. It should be immediately obvious this is not a RCT. It is another modelling study. It is for a very limited location (North Carolina) and cannot be used to to extend beyond 9 months. Let us continue.
“VACCINE EFFECTIVENESS AGAINST HOSPITALIZATION AND DEATH
Many persons with Covid-19 were not contacted for information about clinical outcomes. Therefore, a high percentage of the data regarding hospitalization and death was missing. The percentage of persons who were reached for an interview varied over time and was generally lower during peaks of Covid-19 activity. In addition, reporting of data regarding hospitalization and death was often considerably delayed. Thus, the percentage of missing data was high in the winter and was highest during the last 2 months of the study period”
That is a very glaring limitation.
“Estimates of vaccine effectiveness in reducing the current risk of death due to Covid-19 are shown in Figure 1C and Table 2. For the BNT162b2 two-dose regimen, vaccine effectiveness reached 98.0% (95% CI, 95.5 to 99.1) at 2 months and remained at 90.5% (95% CI, 87.0 to 93.1) at 7 months. For the mRNA-1273 two-dose regimen, vaccine effectiveness reached 98.6% (95% CI, 97.3 to 99.3) at 2 months and remained at 95.5% (95% CI, 93.4 to 96.9) at 7 months. For the Ad26.COV2.S one-dose regimen, vaccine effectiveness reached 85.9% (95% CI, 49.3 to 96.1) at 3 months and was mostly higher than 70% through 6 months, with wide confidence intervals. For all three vaccines, effectiveness tended to be lower among adults 65 years of age or older than among adults 18 to 64 years of age.”
“Our study was observational and thus was limited by confounding bias. We adjusted for measured confounders (age, sex, race or ethnic group, geographic region, and county-level vaccination rate). Of greater importance, we measured the time to disease occurrence from the start of the study in order to compare disease incidence between vaccinated and unvaccinated persons on the same date, thus avoiding confounding due to time trends (e.g., level of community transmission and prevalence of new variants). However, persons who choose not to be vaccinated may differ from those who choose to be vaccinated in terms of their use of other prevention measures. In addition, persons who have Covid-19 symptoms may delay vaccination. It would be difficult to quantify the potential bias caused by these confounding factors”
Ok. 98% effective against death is very high. Again these are just estimates. Do you need to see the Cleveland Clinic graph again to see the real world data against infections?
There is the reality. Increased doses equals more infections in a dose response. How could it possibly increase infection yet prevent death? source
Let us move on to their last reference #17. source
“Viral vector vaccines decreased mortality (risk ratio, 0.25 [95% CI 0.09 to 0.67]; 67 563 participants; 3 trials, low certainty), but comparable data on inactivated, mRNA, and protein subunit vaccines were imprecise. None of the vaccines showed evidence of a difference on serious adverse events, but observational evidence suggested rare serious adverse events”
Imprecise? Please quantify and why is this the opposite conclusion as the study 16 above?
mRNA vaccines.
Five trials assessing mRNA vaccines reported on all-cause mortality. Meta-analysis (RE) showed that these vaccines versus placebo may reduce all-cause mortality, but the confidence interval was compatible with no effect (RR, 0.63 [95% CI 0.21 to 1.84]; p = 0.39; I2 = 0%; 75 926 participants; low certainty)”
WOW compatible with no effect. And that is with low certainty evidence at serious risk of bias and imprecision.
“All the individual vaccines except NVX-CoV2373-Novavax and Gam-COVID-Vac-Sputnik-V may decrease mortality, but their confidence intervals were compatible with no effect: Ad26.COV2.S-Janssen (RR, 0.19 [95% CI, 0.01 to 6.65]), ChAdOx1 nCoV-19-Vaxzevria (RR, 0.21 [95% CI, 0.00 to 55.07]), BNT162b2-Corminarty (RR, 0.50 [95% CI 0.00 to 52.70]), CoronaVac (RR, 0.50 [95% CI 0.03 to 7.35]), mRNA-1273-Spikevax (RR, 0.67 [95% CI 0.01 to 37.52]), NVX-CoV2373-Novavax (RR, 1.00 [95% CI 0.00 to 218.18]), and Gam-COVID-Vac-Sputnik-V (RR, 0.99 [95% CI 0.08 to 244.08). CINeMA was very low for all comparisons (S1 File). The between-study variance could not be estimated due to the small number of trials per vaccine comparison.”
So no effect on mortality. So did not save lives. Even with wishful thinking and low quality evidence. What an abject failure and embarrassment. Back to our original study that wants to compare their results to another study.
The most-cited study is another modelling study. Do we even bother to check it out? I cant help myself.
Another Epstein..I mean Bill Gates funded study! This is what all the pro-vaxx cult followers like to cite. I say let them enjoy it and learn the hard way as long as they do not mandate it or shed it on us.
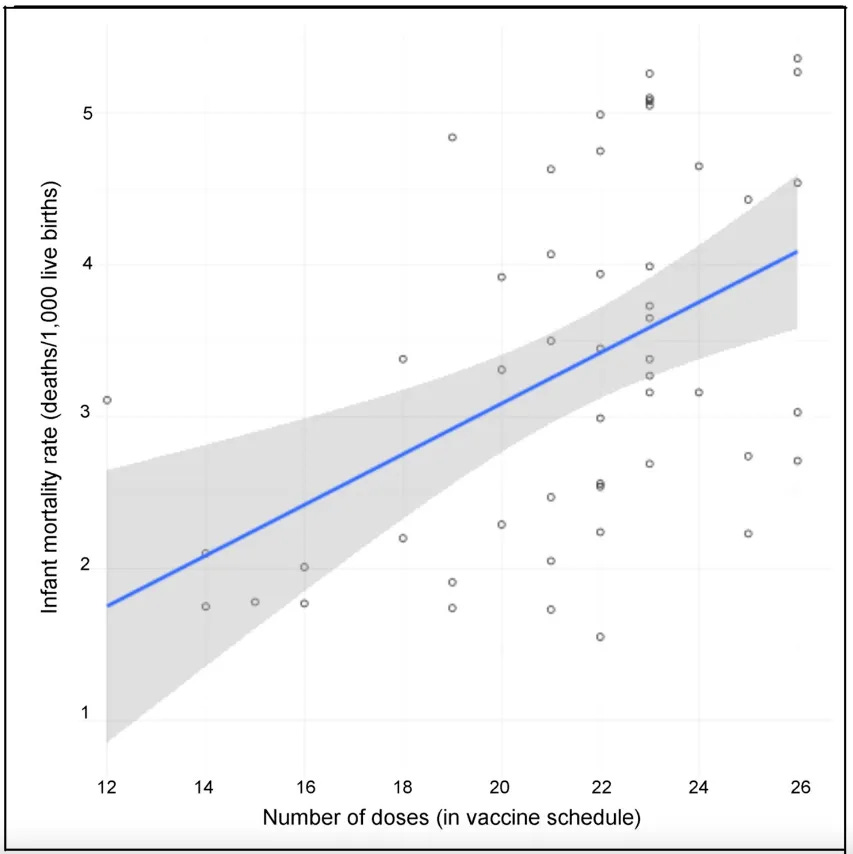
For those that want a study not funded by Bill Gates this is what doses on the schedule plotted against infant mortality rate look like.
In conclusion, the only scientific data that says vaccines save lives are directly funded by Bill Gates and are of low quality and severe risk of bias and are equivalent to wishful thinking and fantasy models for investors and do not count as evidence according to the hierarchy of evidence based medicine.
The medical journals refuse to present information using an absolute risk reduction or number needed to treat to prevent mortality yet make categorical and sweeping statements of causality that they “saved millions of lives”. The entire schedule besides covid did not use an inert placebo and refused to use a meaningful outcome measure like preventing death in their clinical trials. Antibody studies do not constitute proof of benefit against death and are in fact meaningless to harmful for their false sense of assurance and lack of correlate of protection.
The randomized studies show an increased rate of cardiac death which is consistent with the real world data and an abject failure injection that demands 10 doses in the face of rising all cause mortality and collapsed fertility rates.
The reader should be more critical of claims of benefit than claims of harm to avoid damaging the public with unavoidably unsafe vaccines.
I am happy for the doctor-priests that insist on denying the scientific evidence and dying on the metaphorical hill of vaccines. I will enjoy watching.
The claim vaccines save lives including the childhood schedule has been completely discredited.
“The major declines in child mortality that occurred in the first third of the 20th century have been attributable to a combination of improved socioeconomic conditions in this country and the public health strategies to protect the health of Americans. These public health measures included the establishment of local health departments in nearly all of the states. State and local health departments implemented these public health measures including water treatment, food safety, organized solid waste disposal, and public education about hygienic practices. These improvements in water and food safety and purity are linked to the major decline in diarrheal diseases seen in the early years of the century.
Similarly, improvements in housing and decreased crowding in US cities are linked to the reductions in mortality from tuberculosis and other diseases attributable to person-to-person airborne transmission.
Vaccination, while first used in the 18th century, became more widely implemented in the middle part of the century. Vaccines against diphtheria, tetanus, and pertussis became available during the late 1920s but only widely used in routine pediatric practice after World War II. Thus vaccination does not account for the impressive declines in mortality seen in the first half of the century.”

























Wonderful article