


Covid quacksines cause cancer
confirmatory update


The scientific literature confirms what everyone suspects. The poison-19 injections cause cancer.

Statistically significant increases in age-adjusted mortality rates of all cancer and some specific types of cancer, namely, ovarian cancer, leukemia, prostate, lip/oral/pharyngeal, pancreatic, and breast cancers, were observed in 2022 after two-thirds of the Japanese population had received the third or later dose of SARS-CoV-2 mRNA-LNP vaccine. These particularly marked increases in mortality rates of these ERα-sensitive cancers may be attributable to several mechanisms of the mRNA-LNP vaccination rather than COVID-19 infection itself or reduced cancer care due to the lockdown. The significance of this possibility warrants further studies.
Mortality from all cancers did not increase in 2020…The restrictions on access to cancer screening or treatment seem to have been much relieved after late 2021. Mass vaccination with the first and second doses started in the spring of 2021, and the vaccination rate soon peaked in the summer of 2021 at 80% of the population. The vaccination rate for the third dose peaked in the spring of 2022, at 68%. Now, Japan is even conducting mass vaccination with a seventh dose, making it the country with the highest vaccination rates.
Researchers have reported that the SARS-CoV-2 mRNA-LNP vaccine may pose the risk of development and progression of cancer [25-28]. In addition, several case reports have described cancer developing or worsening after vaccination and discussed possible causal links between cancer and mRNA-LNP vaccination [29-34].
Based on the molecular weight of BNT162b2 mRNA (Pfizer-BioNTech), the mRNA content per dose is estimated at 13 trillion molecules and 40 trillion molecules in mRNA-1273 (Moderna) [35,36]. The total number of cells in humans is estimated to be 37.2 trillion [37], making the number of mRNA-LNPs very high, ranging from one-third to the equivalent of the total cell number. After inoculation, the mRNA-LNPs are delivered to various organs, especially the liver, spleen, adrenal gland, ovary, and bone marrow [38]. In one study, vaccine mRNA was detected in the lymph nodes of persons vaccinated with hybridization of a SARS-CoV-2 mRNA vaccine-specific probe 7 to 60 days after the second mRNA-1273 or BNT162b2 dose [39]. Modified mRNA with N1-methyl-pseudouridine could translate a large amount of SARS-CoV-2 spike protein (S-protein) [40]. S-protein emerged on the surface of exosomes in the blood of the vaccinated [41]. Fragments of vaccine-specific recombinant S-protein were found in blood specimens of 50% of vaccine recipients and were still detected three to six months later [42].
Cancer development by SARS-CoV-2 mRNA vaccine
In our study, the AMRs of ovarian cancer, leukemia, prostate, lip/oral/pharyngeal, pancreatic, and breast cancers increased significantly beyond the predicted rates, especially in 2022. All of these cancers are known as estrogen and estrogen receptor alpha (ERα)-sensitive cancers [78-83]. Recent research by Solis et al. on the binding ability of S-protein of SARS-CoV-2 against over 9,000 human proteins has shown that S-protein specifically binds to ERα and upregulates the transcriptional activity of ERα. The addition of estradiol (E2) to human breast cancer cells causes proliferation of the cancer cells, whereas the addition of raloxifene, a selective ERα modulator, inhibits proliferation. Breast cancer cells grow when S is added instead of E2, and the addition of raloxifene inhibits their growth. Solis et al. also mentioned that the finding of S-ERα cytosolic colocalization may lead to a potentiation of membrane-bound ERα signaling [84]. Membrane-bound ERα has been implicated in many pathways, including the activation of c-Myc, which promotes the cell cycle and impacts cancer development [85].
ERα-mediated transcription may induce endogenous DNA double-strand breaks (DSBs) in ER-sensitive cancers [86]. Studies have shown that transcriptionally activated ERα induces DSBs by topoisomerase II and the recently known R-loop/G-quadruplex structures formation, significantly increasing the need for BRCA1 for their repair in breast cancer cells [87-89]. One study showed nuclear translocation of mRNA and S protein with the nuclear localization signal [90], and an in silico bioinformatic analysis showed interactions between the S2 subunit of S-protein and BRCA1, BRCA2, and P53 [91], possibly resulting in their sequestration and dysfunction. The possible co-occurrence of high BRCA1 demand to repair DNA damage caused by activated transcription via ERα bound with S-protein along with dysfunction of BRCA1 sequestrated by S-protein raises concerns about increased cancer risk in ERα-sensitive cells in mRNA-LNP SARS-CoV-2 vaccine recipients.
As mentioned above, there is also great concern about the risk of dysfunction in the crucial cancer suppressor genes, brca2 and P53, as well as BRCA1, through mechanisms involving downregulation of IRF9 through interference by specific miRNA in exosomes [26] and the possible sequestration by the S2 subunit of S-protein in the vaccine [91]. Impaired BRCA1 activity is associated with higher risk of breast, uterine, and ovarian cancer in women and prostate cancer in men, as well as moderately higher risk of pancreatic cancer in both men and women [92]. BRCA2-associated cancers include breast and ovarian cancer in women, prostate and breast cancer in men, and acute myeloid leukemia in children [26]. These findings are highly consistent with our results.
Additional factors that may contribute to the development of cancer are being investigated. Since endogenous ROS causes oxidative DNA damage [93], excessive oxidative stress resulting from the downregulation of ACE2 by S-protein [57] may contribute to cancer development. One study showed that the downregulation of the Mas receptor promotes the metastasis of epithelial ovarian cancer [94]. ACE2 receptor, bound by S-protein after mRNA-LNP vaccination, may directly cause downregulation and subsequent dysfunction of the Mas receptor, possibly leading to an increased risk of metastasis in vaccinated women with ovarian cancer. The observation that injected LNPs accumulate particularly in the ovaries and bone marrow [38] could better explain our findings of excess mortalities from ovarian cancer and leukemia in 2022. According to an analysis of scientific literature about sex hormone receptors in head and neck squamous cell carcinoma (HNSCC), ERα plays various roles in the biopathology of HNSCC, particularly oropharyngeal cancer. These include promoting DNA hypermutation, facilitating HPV integration, and cooperating with epithelial growth factor receptor (EGFR) [82]. This may explain the increased mortality of lip/oral/pharyngeal cancer in our study.
A recent study showed that SARS-CoV-2 RNA could be reverse-transcribed to DNA and integrated into the human cell genome in vitro [95]. Another study reported that transfected mRNA in the human cells exposed to BNT162b2 leads to unsilencing of the endogenous retrotransposon long interspersed element-1 (LINE-1) and reverse transcription of vaccine mRNA sequences to DNA in the nucleus [96]. Accumulation of vaccine mRNA and reverse-transcribed DNA molecules in the cytoplasm could be expected to induce chronic autoinflammation, autoimmunity, DNA damage, and cancer risk in susceptible individuals [97].
The U.S. Food and Drug Administration (FDA) states in its guidance for the production of viral vaccines for infectious disease, "There are several potential mechanisms by which residual DNA could be oncogenic, including the integration and expression of encoded oncogenes or insertional mutagenesis following DNA integration" [98]. The FDA's guidelines are essential for Japan because Japan's special emergency use authorization depended on FDA approval during the COVID-19 pandemic [99]. Recently, some researchers have reported that several lots of Pfizer-BioNTech and Moderna vaccines contain a certain amount of double-stranded DNA fragments from residual plasmid vectors [100,101]. Some of them mentioned that the amount of residual DNA exceeds the regulatory limits for residual DNA set by the FDA. Given these reports and the FDA's regulatory statement, further investigation is required to determine whether the observed excess cancer deaths following mass vaccination were linked to reported residual DNA in the vaccine.

To study the effect of spike S2 on p53 activity as would occur after virus entry into host cells, we transiently transfected SARS-CoV-2 spike S2 subunit into cancer cells thereby avoiding possible effects of a virus infection or cell-cell fusion on p53 signaling. Our findings agree with previous results showing that spike could not stabilize p53 in low ACE2 cells that are unable to undergo cell-cell fusion [9].
The p53 protein is considered as a “genome guardian” by arresting the cell cycle to repair DNA damage or causing cell death in the presence of unrepaired persistent damage and stress [14]. In our preliminary experiments reported here, the SARS-CoV-2 spike-induced inactivation of p53 was correlated to an apparent reduction of expression of DNA damage response protein γ-H2AX after cisplatin exposure and a reduced cell cycle checkpoint response in the cancer cells (Figure 3). Whether these changes are a consequence from the suppressive effect of SARS-CoV-2 spike S2 on p53 signaling in cancer cells needs to be further investigated.
Our results have implications for the biological effects of spike S2 subunit in human cells whether spike is present due to primary COVID-19 infection or due to mRNA vaccines where its expression is used to promote anti-viral immunity. A perturbed p53 pathway is concerning but also complicated in sorting out since cellular transformation and cancer are a multi-step process that evolves over time.

Despite the assumption that there is no possibility of genomic integration of therapeutic synthetic mRNA, only one recent study has examined interactions between vaccine mRNA and the genome of transfected cells, and reported that an endogenous retrotransposon, LINE-1 is unsilenced following mRNA entry to the cell, leading to reverse transcription of full length vaccine mRNA sequences, and nuclear entry. This finding should be a major safety concern, given the possibility of synthetic mRNA-driven epigenetic and genomic modifications arising. We propose that in susceptible individuals, cytosolic clearance of nucleotide modified synthetic (nms-mRNAs) is impeded. Sustained presence of nms-mRNA in the cytoplasm deregulates and activates endogenous transposable elements (TEs), causing some of the mRNA copies to be reverse transcribed. The cytosolic accumulation of the nms-mRNA and the reverse transcribed cDNA molecules activates RNA and DNA sensory pathways. Their concurrent activation initiates a synchronized innate response against non-self nucleic acids, prompting type-I interferon and pro-inflammatory cytokine production which, if unregulated, leads to autoinflammatory and autoimmune conditions, while activated TEs increase the risk of insertional mutagenesis of the reverse transcribed molecules, which can disrupt coding regions, enhance the risk of mutations in tumour suppressor genes, and lead to sustained DNA damage. Susceptible individuals would then expectedly have an increased risk of DNA damage, chronic autoinflammation, autoimmunity and cancer. In light of the current mass administration of nms-mRNA vaccines, it is essential and urgent to fully understand the intracellular cascades initiated by cellular uptake of synthetic mRNA and the consequences of these molecular events. source


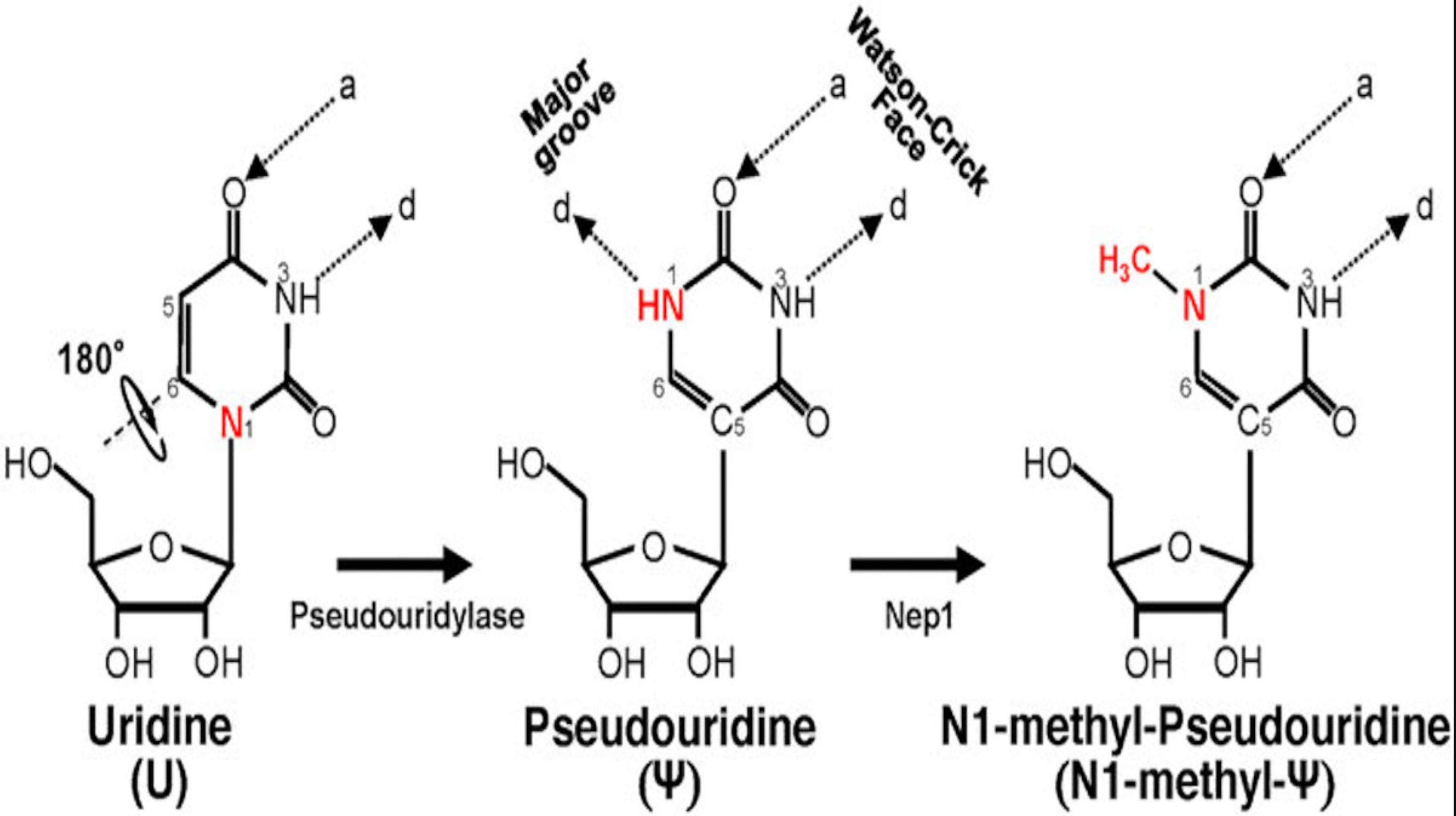
This is the vile lying Nobel Prize winning traitor saying N1 methylpseudouridine is identical to the mRNA in your cells. He is a pathological liar and should be prosecuted for bioterrorism.
With generous support from moderna. I bet.


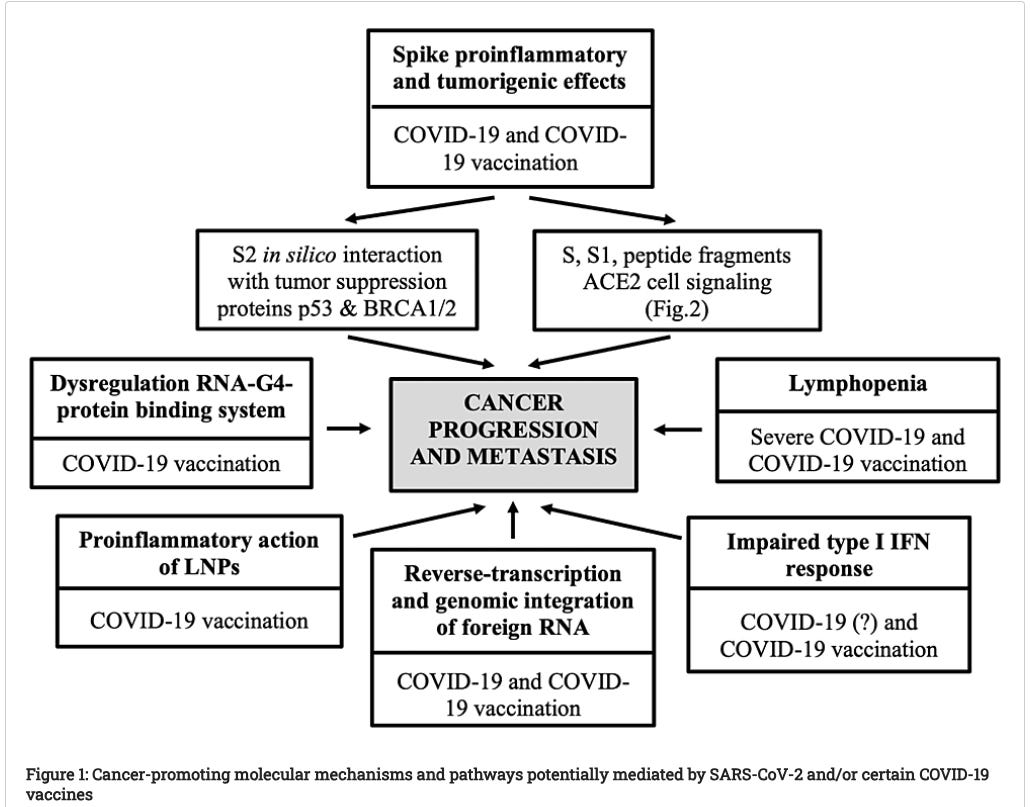
SARS-CoV-2 spike glycoprotein-based vaccines, particularly mRNA vaccines, have the potential to initiate a set of biological mechanisms that may collectively generate a (transient) pro-tumorigenic environment favorable to cancer progression and/or reactivation of DCCs. These adverse effects may be attributed to the pro-inflammatory action of the lipid nanoparticles (LNPs), the impaired type I interferon (IFN) response, the translational dysregulation of cellular microRNAs triggered by structurally modified mRNA (mRNA vaccines), and/or the unique nature, expression pattern, binding profile, and pro-inflammatory and tumorigenic effects of the produced antigens, namely, the SARS-CoV-2 spike protein and/or its subunits S1 and S2 (mRNA and adenovirus-vectorized vaccines)

Conclusion
TNFα appears to be the primary cytokine in the pathogenesis of Covid-19 in all its forms and the associated risks of cancer, autoimmunity, and fibrosis. It promotes the high mannose glycosylation of CD147. Overexpression of CD147 is linked with tumorigenesis and tumor progression, i.e., local spread, metastasis, poor prognosis, and resistance to chemotherapy. TNFα promotes the high mannose glycosylation of the TGF beta receptor. This in concert with EMMPRIN aka CD147 facilitates EMT, EndMT, and CAF, affiliated with both organ fibrosis and tumor spread. CD147 in concert with Th17 triggers the secretion of IL17 and IFN gamma, tightly linked to autoimmune disease.
TNFα, produced by TACE aka ADAM17, is upregulated when SARS CoV2 enters the cell endocytotically or when AT1Rs are activated by any means (see figure 1).
Elevated TNFα is linked with aggressive TNBC and aggressive colon cancers. The former is more commonly encountered in women under 40, African Americans, Hispanics, the obese, the vitamin D deficient, and the magnesium deficient. Both are claimed to be vaccine induced turbo cancers. If the presented scenario based on the most recent physiologic findings is correct, then the repeated doses of the vaccine and the recurrent infections they enable (see figure 2) both stoke repeated exposures to elevated TNFα. In those susceptible, as described, these exposures carry great risk.

There is limited information to make a safety assessment of mRNA vaccines. In the category of mRNA vaccines, there are patient data for 385 patients. For mRNA vaccines against an infection, there are data for 285 patients. The rate of serious adverse events was 64 out of 385 for the broad category of RNA vaccines (including cancer vaccines), or 17%; restricting the definition to vaccines against infection, the rate of SAEs is 41/285 or 14%. While high levels can be expected for trials of a novel technology where dosage levels must be determined (many of these trials are phase I) [177], these findings showcase the relative immaturity of mRNA vaccination as a strategy. Given the low efficacy and short duration of protection of SARS-CoV-2 mRNA products [178,179], and the low risk of many populations from COVID-19 complications [180], it may be advisable to suspend mRNA vaccines in certain risk cohorts.
The key to the reactivity of mRNA vaccines is the fact that they express a foreign antigen, for which the antigen-presenting cells are marked for destruction. While the lipid nanoparticle exhibits an acute inflammatory response by itself [77,78,181], the trials using LNPs, so far, have not found a large safety signal when using LNPs to deliver small molecules, non-expressing RNAs, or RNAs for endogenous proteins [77,78,181].
In addition to there being harms attributable to the general immune response from an LNP–RNA delivery system, there are also some harms specific to the spike protein. Several of these mechanisms are supported by laboratory experiments and clinical findings, but need more investigation. Medicine is replete with cases for which safety was assumed without adequate evidence at the time, which later regretfully led to loss of health and life. mRNA vaccines are demonstrating great unintended harms, and these harms demand further investigation into the mechanisms, which is important for identifying treatment modalities.

There is concern that COVID-19 vaccination per se might contribute to long COVID, giving rise to the colloquial term ‘Long Vax(x)’.22 The spike protein of SARS-CoV-2 exhibits pathogenic characteristics and is a possible cause of post-acute sequelae after SARS-CoV-2 infection or COVID-19 vaccination. COVID-19 vaccines utilise a modified, stabilised prefusion spike protein that might share similar toxic effects with its viral counterpart.22,23 A possible association between COVID-19 vaccination and the incidence of POTS has been demonstrated in a cohort of 284,592 COVID-19-vaccinated individuals, though at a rate that was one-fifth of the incidence of POTS after SARS-CoV-2 infection.24 Multiple studies have shown an increased risk of myocarditis after vaccination with mRNA encoding SARS-CoV-2 spike protein.25–27 mRNA vaccines can result in spike protein expression in muscle tissue, the lymphatic system, cardiomyocytes and other cells after entry into the circulation.28 Recipients of two or more injections of the mRNA vaccines display a class switch to IgG4 antibodies. Abnormally high levels of IgG4 might cause autoimmune diseases, promote cancer growth, autoimmune myocarditis and other IgG 4-related diseases (IgG4-RD) in susceptible individuals.29 There are clear implications for vaccine boosting where these and similar observations8,22,30 relating to COVID-19 vaccination and the incidence of long COVID-like symptoms are substantiated, adding further to public health officials’ concerns. Understanding the persistence of viral mRNA and viral protein and their cellular pathological effects after vaccination with and without infection is clearly required. Because COVID-19 vaccines were approved without long-term safety data and might cause immune dysfunction, it is perhaps premature to assume that past SARS-CoV-2 infection is the sole common factor in long COVID.8


New Case Studies:

Hemophagocytic lymphohistiocytosis (HLH) has been recognized as a rare adverse event following the coronavirus disease 2019 (COVID-19) vaccination. We report a case of neuropsychiatric symptoms and refractory HLH in a woman with systemic lupus erythematosus (SLE) after receiving her COVID-19 vaccine treated with belimumab, later found to have intravascular large B-cell lymphoma (IVLBCL) at autopsy. A 61-year-old woman with SLE was referred to our hospital because of impaired consciousness and fever. One month prior to consulting, she received her second COVID-19 vaccine dose. Afterward, her consciousness level decreased, and she developed a high fever. She tested negative for SARS-CoV-2. Neuropsychiatric SLE was suspected; therefore, glucocorticoid pulse therapy was initiated on day 1 and 8. She had thrombocytopenia, increased serum ferritin levels and hemophagocytosis. The patient was diagnosed with HLH and treated with etoposide, dexamethasone and cyclosporine. Despite treatment, the patient died on day 75; autopsy report findings suggested IVLBCL as the underlying cause of HLH. Differentiating comorbid conditions remains difficult; however, in the case of an atypical clinical presentation, other causes should be considered. Therefore, we speculate that the COVID-19 vaccination and her autoimmune condition may have expedited IVLBCL development.


Apply the Bradford Hill criteria to modmRNA-LNP injection and cancer.
There is a strong increase in signal /effect size. Cancer is going up in all monitoring systems.
This result is consistent. Cancer is increasing everywhere from the United States to Japan.
It is specific to anyone who took immune suppressing modified mRNA. These signals are not present with the non-mRNA injections.
Normally it takes a long time to develop cancer from a toxic exposure. Take cigarette smoking and development of lung cancer. Not with modmRNA injections. People are getting recurring cancers or new cancers within days. This is not a coincidence.
Biological gradient is satisfied with more doses. There is a clear switch to cancer insulating IgG4 antibodies after the 3rd shot. Japan’s cancer incidence increased after the majority had 3 doses.
I have listed 20 mechanisms of action it could cause cancer. This is extremely plausible.
SARS-CoV-2 Vaccination and Oncogenesis

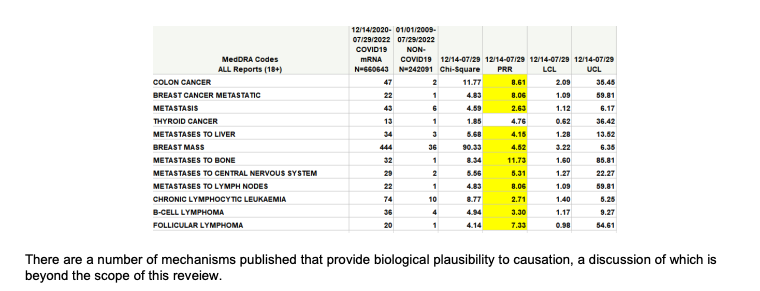
With time more and more adverse events are being slowly acknowledged as being attributed to ill-advised covid EUA DoD countermeasure gene technology injections commonly and incorrectly referred to as vaccines. Recently a large 8 country observational cohort study with
The real world data and scientific literature are coherent. It increases cancer.
Numerous in vitro experiments have shown the mechanisms of DNA integration and replicating in cancer cell lines and human liver cell lines.
Analogy. People with immunosuppression like HIV/AIDS patients have a hard time fighting off cancer. If you turn off cancer surveillance though modified mRNA cancer will increase…
Reversibility. The unvaccinated are not dying of turbo cancer. If we were it would be on the news incessantly.
IT CAUSES CANCER.
I have a friend whose college-age son developed leukemia shortly after the mRNA injections. He still thinks it's a "conspiracy theory" that the injection could be related.
It's all very sad.
Never in my life in a two year period have I known 9 people with a cancer diagnosis 5 have since died.